
In 2007 my beloved son Andrew Black was unlawfully killed by
VCJD/Human BSE, know as the human form of mad cow disease.
He was just 24 years old. Since his untimely and avoidable
death I created a campaign to find out why my Andrew died
and who is responsible. Food and medicines should be safe and never kill.
This is my blog containing the history of my investigations, facts and information the UK
government have tried to supress. It is the history of my ongoing investigations, and how
millions of us remain at risk of developing Human BSE. The disease has not gone away
and continues to kill people and animals globally in 2017.
CHRISTINES BLOG
MONDAY 2ND SEPTEMER 2024
Today is when my son Andrew was born in 1983. His life cut short at 24 years old as he was unlawfully killed by the deliberate decisions of the UK government and its ministers, who I name and shame on Andrews website. Human BSE, the human form of mad cow disease was a preventable mad made zoonotic disease, with human, animal health bottom of the list and profit, ministerial careers before my sons life and well-being. Millions of us have been exposed to the same lethal pathogen which killed my only son Andrew.
Below is a poem I wrote, just days after Andrew died a very painful death, at just 24 years old. A career in the media, he was a well respected professional across all media, radio and tv. Time does not heal but, I smile remembering my Andrew, and his loving, gentle nature and contribution to this world.
MY LOST BOY
By Christine Lord
When you have gone far, far away,
from my embrace and care,
I will feel your warmth the smell of newly washed hair.
and smile
When you have gone far, far away,
from my eyes eagle view,
I will see you handsome, designer dressed top to toe.
and smile.
When you have gone far, far away,
from an mothers words pf advice, concern.
I will hear your deep laughter, chuckling grin.
and smile.
When you have gone far, far away,
from more birthdays, Christmas and days of light,
I will remember a child’s chubby hand, kisses hello.
and smile.
When you have gone, far, far away
my beloved beautiful boy,
the part of me that is you and I
will remain a heartbeat away.
AND I WILL SMILE.
WEDNESDAY JULY 24TH 2024
There has been a record number of people diagnosed with dementia in England during the past year. Please see the article from the Guardian below. All of these people would have been exposed to high levels of BSE mad cow disease infected material. Lethal BSE material, was in everything from baby cough medicine, contact lens solution, make-up and of course school meals, supermarket food, medicines.
Many cases of dementia are no longer in the elderly but relatively much younger patients. Lancet 2012, research, found that 1/2,000 of the UK population now carry or incubate the human form of mad cow disease. It can have between 10 to 50 years incubation.
One of the terrifying symptoms of human mad cow disease is dementia. When I took my increasingly unwell only son Andrew Black, aged 23, to a host of GPS, Consultants they diagnosed depression. It was only due to my journalism skills/knowledge about BSE/vCJD/Prion Disease that I told the neurologist, I suspected Andrew had been infected with human BSE. Only then were numerous tests carried out on my young son. Vegetarians/Hindus have also died of human BSE too. We as a family had not eaten beef/beef products since Andrew was 6 years old.
The results from neurology within a week confirmed that my son had Human BSE and had just 6 months to live. Just a few months before Andrew had produced perfectly his last radio show for talkSPORT. Within months Andrew was blind, quadriplegic, unable to eat, or recognise friends. Please read my book, available Amazon, Who killed my son? and read my real time diaries I kept during Andrews last days and my investigations as a journalist since. How I was intimidated/threatened off camera during an interview for BBC1 by a high level minister, who I name in my book. He now resides in the House of Lords. This was just 16 weeks after my son Andrew had died in my arms. This Minister who was responsible for allowing infected BSE to saturate our food and medicine supply for years, is also profiled on my main website, John Gummer.
As a journalist I continue to reveal the truth about the food we eat, politicians we vote for and the scientists who we trust.
Thank you Christine

Record numbers of people in England given dementia diagnosis in past year
MONDAY 29TH APRIL 2024
https://mail.aol.com/d/list/referrer=newMail&folders=1&accountIds=1&listFilter=NEWMAIL/messages/AM39NkxW7EXVZi3s_wSnaEocEDE#:~:text=https%3A//www.independent.co.uk/news/science/bird%2Dflu%2Dmilk%2Dcows%2Davian%2Dinfluenza%2Db2535749.html
Please listen to BBC Sounds, ‘The Cows are Mad’, where I talk about not ‘if’ but ‘when’ we may face the next human global pandemic. Due to disease spread from animals to humans, caused through global governments food policies supporting big corporations profits rather than human, animal, climate health.
https://www.independent.co.uk/news/science/bird-flu-milk-cows-avian-influenza-b2535749.html
WEDNESDAY 6th MARCH 2024
‘The English Erin Brockovich’ ‘
‘Who Killed My Son? is at once a page-turning thriller & urgent piece investigative journalism & should be read by anyone who cares about food they eat, politicians they elect, scientists they place their trust in.’ Review NUJ, Prof Tom Skykes.
Please read my book and see how 16 weeks after the unlawful death of my only son Andrew Black aged 24, due to human form of mad cows disease. John Gummer, Minister of Agriculture BSE epidemic, during my explosive BBC1 interview with this Minister, off camera threatened me and try to silence me and my investigations.
The Cows are Mad, BBC Radio 4 podcast/BBC sounds. Available now.
bbc.co.uk/programmes/m001rrhy… Over 3 million listeners & rising, my research & book, Who Killed my Son? weave throughout this podcast. I feature in episodes 4, 6 ,10. Please share. BSE the harbinger of Covid and unfortunately future pandemics.
 John Gummer continues to profit from the cover-ups surrounding BSE and the human form mad cow disease. ‘Reputation Washing.’
John Gummer continues to profit from the cover-ups surrounding BSE and the human form mad cow disease. ‘Reputation Washing.’
SATURDAY 16TH DECEMBER 2023
On 16th December 2007 my beautiful, strong, son Andrew Black was unlawfully killed by the human form of BSE, known as Mad Cow Disease. He was just 24. Lancet 2012 (1 in 2,000 of UK population incubate, carry Human BSE)
Andrew was a rising star in the media, producer, TalkSport, BBC, SKY, ITV. From living a great life in London and Manchester within months he was quadriplegic, blind, unable to recognise friends.
Andrew had not eaten beef/beef products since he was 4 years of age. Human BSE like Covid is a zoonotic avoidable disease, transferred from animals to humans. I buried my only violet eyed, handsome son just 3 days before Xmas.
As an investigative journalist, I have spent decades uncovering the truth
I have been threatened, scorned by the establishment. If you care about the food you eat, the scientists in whom you trust, the politicians who you vote for please read my book ‘Who Killed my Son?’ Amazon Books and listen to the BBC Podcast The Cows are Mad. I feature in episodes 4, 6 and 10.
As Christmas approaches spare a thought for all the bereaved, especially this time of year and every year, and give your family, friends and colleagues that extra hug. Andrew could be anyone’s son, brother, friend or family member it could be you. BSE was the harbinger of Covid and unfortunately future pandemics will be heading our way, unless political policy reflects concern for our environment, human and animal welfare.
Thank you, for reading this. Christine Lord

Andrew ‘legend of the desk’ working as producer at talkSPORT aged 22
WEDNESDAY 15TH NOVEMBER 2023
If you care about the food you eat, the politicians who you vote for and the scientists in who you place your trust, please listen to Radio 4, BBC Podcast, The Cows are Mad. Listen to John Gummers comment, that human mad cow disease, may not have come from eating BEEF?
My 17 year investigations into the BSE epidemic, harbinger of covid and future pandemics, and BSE’s ongoing consequences for everyone, are explored in Episode 4,6 and 10.
To find out more about the threats to my well-being, the cover-ups and lies surrounding human mad cow disease please read my Amazon books, ‘Who killed my son?’.
Thank you. Christine Lord
https://www.bbc.co.uk/sounds/brand/m001rrhy?partner=uk.co.bbc&origin=share-mobile
THURSDAY 19th October 2023
If you care about the food you eat, the politicians you vote for and the scientists in whom you place your trust. Please listen to my story on BBC podcast,’ The Cows are Mad’, a ten part series for Radio 4, beginning Monday October 23rd 1.45pm. All episodes available BBC sounds.
The Cows are Mad, Producer Lucy Proctor
https://www.bbc.co.uk/programmes/m001ryb4
SATURDAY 2nd SEPTEMBER 2023
Today is my only son Andrew’s birthday, no cake, no hugs, just tears. Andrew was unlawfully killed by human form of mad cow disease at just 24 years old. Our family had not eaten beef/beef products since he was tiny. Read my expose/govt cover-ups, lies, threats, to this journalist/grieving mother. Who Killed my son? Amazon. Love you Andrew always forever x

Andrew far left happier times with his best friends
MONDAY 5TH June 2023
APOLOGIES TO PEOPLE WHO ARE TRYING TO READ THE MAIN WEBSITE, ONCE AGAIN AS MY INVESTIGATIONS GET CLOSER TO THE TRUTH, THE WEBSITE HAS BEEN HACKED WITH IMPORTANT INFORMATION REMOVED. DONT WORRY WE ARE WORKNG ON THIS…Christine Lord
THURSDAY 1ST JUNE 2023
https://www.mirror.co.uk/news/us-news/extremely-rare-case-mad-cow-30073354
The article above from todays Mirror, newspaper, explores how a cow in the US was found to be infected with BSE, Mad Cow disease. Below are the latest figures from my research about the numbers of cattle in the USA , the numbers annually tested for BSE.
There are 89.3 million US cattle (1/01/2023) just 25,000 USA cattle tested yearly for BSE. How many cows infected with human mad cow disease, are still entering USA and global food chain? ‘Downer cattle’ cows that just collapse and die, often enter the US food chain, with no questions asked. How many US cows infected with mad cow disease continue to enter USA and global food chain?
Is this why so many people within the global population are getting strange dementia type disease? We face a pandemic of dementia diseases across the world in often younger people too!
WEDNESDAY 3rd May 2023
BSE fears in Taiwan, over lifting of Canadian Beef ban.
https://focustaiwan.tw/society/202305010007
Consumers’ Foundation opposes lifting ban on older Canadian beef

A worker puts beef slices into a pot of broth during a cooking demonstration held by trade promotion group Canadian Beef in Kaohsiung in 2009. Taiwan first banned all imports of Canadian beef in 2003 before partially lifting the ban on boneless meat in 2007. CNA file photo
Taipei, May 1 (CNA) The Consumers’ Foundation voiced its opposition Monday to the government’s plan to lift a ban on Canadian beef over 30 months old because Canada reported a case of mad cow disease as recently as just over a year ago.
A case of bovine spongiform encephalopathy (BSE) was reported in Canadian cattle in December 2021, prompting South Korea to suspend beef imports from the North American country, the nonprofit group said in a statement.
China and the Philippines later followed suit, it said.
It has barely been a year since BSE was last reported in Canada, and doubts about the safety of cattle feed have yet to be answered, the foundation said, referring to BSE cases in Canada in 2015 which were later been found linked to contaminated feed.
If Taiwan’s Food and Drug Administration (FDA) insists on disregarding public opinion by lifting the ban on Canadian beef over 30 months old, the foundation said it will call on consumers to initiate a boycott against imports of that type of beef.
Currently, Taiwan only imports beef from Canada under 30 months old. It lifted restrictions on imports of United States beef from cattle slaughtered after the age of 30 months on Jan. 1, 2021.
Because of the relatively long incubation period of mad cow disease, cows aged 30 months or less are generally thought to be at lower risk of having the disease than cows older than 30 months of age.
Feed can also be made from parts of the cow considered to be at highest risk of BSE, such as the spinal cord and brain, from cows over 30 months old.
Last week, the FDA issued an advance notice that Taiwan will lift a ban on imports of beef from Canada over the age of 30 months.
The notice was issued on April 27 and will remain active for 30 days to give the public time to comment on the matter, according to the FDA, but whether it will listen to opposing voices such as the Consumers’ Foundation remains to be seen.
The move to allow imports of the beef appears to be economically motivated.
It came after a government source said recently that the ban could be a stumbling block in talks on a bilateral foreign investment promotion and protection agreement (FIPA) between Taipei and Ottawa.
According to Cheng Wei-chih (???), deputy head of the FDA’s Food Safety Division, Canada obtained World Organization for Animal Health negligible risk status for BSE in February.
In response to the foundation’s statement, the FDA on Monday said consumption of Canadian cattle meat posed low health risks to humans.
Based on international statistics, only two out of 10 billion people are at risk of mad cow disease due to the consumption of Canadian beef, which is extremely low, FDA Director-General Wu Show-mei (???) told CNA but did not provide the source for that information.
Wu said the sources of Taiwan’s imported beef and pork were clearly labeled to help consumers make decisions about what to buy.
In the case of Canadian beef over 30 months, it will be subject to the same border inspection regulations as other items imported from other countries, she said.
MONDAY 27th March 2023
https://www.mirror.co.uk/news/uk-news/mad-cow-disease-killing-factory-29502468
https://www.sciencedirect.com/science/article/pii/S0264837722005488
The articles and investigations above highlight the on-going dangers of BSE infected material. BSE infected material can incubate in humans for over 50 years and its lethal abilities to kills can remain in the ground on surfaces for decades possibly forever.
MONDAY 20th MARCH 2023
Mad Cow Disease Found On Farm In Netherlands
Mad Cow Disease Found On Farm In Netherlands

- February 3, 2023
A rare disease that is 100% fatal once symptoms appear has been detected in a cow at a farm in the Netherlands. Worryingly, the disease can be passed to humans when they eat beef of cows contaminated with the disease.
The disease called bovine spongiform encephalopathy (BSE) or more commonly as mad cow disease has been reported in the country for the first time in over a decade.
Authorities believe that the cow is not a threat to human health as it was caught before it entered the food chain. However, they are on the lookout for other animals that have come in contact with the cow or were infected by the same source.
“Offspring, and animals that have had the same feed, and animals that have grown up with this bovine are being tracked down, tested for BSE,” and will be put down, Agriculture Minister Piet Adema said, the NL Times reported. “There is a chance that other cattle have also eaten this feed and become infected from it. In that case, measures must be taken to manage risks to food safety and public health.”
BSE is a type of prion disease infecting cows. Prions are the misfolded forms of naturally occurring proteins. Often found in the brain, these unnatural proteins convert normal proteins when they encounter them. The result is a cascading effect that damages the brain eventually. While different incubation periods exist depending on the disease, currently, all prion diseases are 100% fatal once symptoms appear, according to Gizmodo.
The BSE equivalent in humans is Creutzfeldt-Jakob disease or CJD. Most cases of CJD occur sporadically, usually in later life. Yet other forms of the disease can occur as a result of inherited mutations or contaminated surgical equipment or during certain procedures of organ donation. But it is the form of the disease called variant CJD, which is caught by eating beef contaminated with BSE.
This is not our first encounter with the deadly disease.
Hundreds of people developed variant CJD in the 1980s and 1990s from contaminated beef. Interestingly, most of these cases were in the UK. The outbreak is believed to have been caused due to the practice of feeding cows the meat of other infected cows or even from sheep infected with the prion disease called scrapie, as per the outlet.
After prominent bans on British beef, as well as changes in feeding and slaughter regulations, mad cow disease incidence had decreased by the mid-1990s. Large-scale outbreaks of either BSE or variant CJD have not occurred since then. But BSE can still spontaneously occur in cows on farms, in which case containing it becomes a priority.
MONDAY 17TH OCTOBER 2022
My tweet @justiceandy below, plus the full article from the Guardian newspaper UK. Since Brexit the lowering of food safety standards, put the UK/World at risk of another zoonotic pandemic from diseases transferred from animals to humans.
“The Food Standards Agency (FSA) has lost full access to EU’s rapid alert system on food and feed, which provides information on food safety alerts to member states, it noted.” theguardian.com/politics/2022/ Another pandemic/zoonotic disease waiting in the wings?
https://www.theguardian.com/politics/2022/oct/12/uk-trade-regulators-struggling-cope-poor-brexit-planning-mps-say
UK trade regulators struggling to cope due to poor Brexit planning, MPs say
Commons committee warns there are still shortages of staff to deal with UK’s new status as a third country.
UK regulators are struggling to cope with the post-Brexit trading environment because of “poor preparation and planning”, a House of Commons committee investigation has found.
Almost two years after the UK quit the EU, there are still shortages of vets, toxicologists, lawyers and economists to deal with the UK’s new status as a “third country”, found the public accounts committee report, Regulating After EU Exit.
And it warned that a mooted 40% head count reduction across government, if implemented, would “make current regulatory models unsustainable” without changes to legislation.
“[The] government’s poor preparation and planning have combined with international political realities and the result is exposure of UK consumers and businesses to greater risks and costs,” said Dame Meg Hillier, the MP who chairs the committee.
The committee, which took detailed evidence from food, competition and chemicals agencies, found the regulators were making good strides towards working with international counterparts.
However, it also noted the effect on industry and consumers after the loss of access to EU data systems.
The Food Standards Agency (FSA) has lost full access to the EU’s rapid alert system on food and feed, which provides information on food safety alerts to member states, it noted.
The lack of membership of the EU’s chemicals regulatory regime, Reach (registration, evaluation, authorisation and restriction of chemicals), will cost an estimated £800m to replicate in a UK-only regime.
“The regulators are taking action to mitigate these issues, but in some instances the alternatives are more time-consuming and are likely to increase costs over time,” the report warned.
The committee’s report found regulators were unable to recruit and retain enough staff skilled in the post-Brexit regime, with trade in farm produce particularly affected because of new veterinary certification needed on exports.
It also warned of dangers to the farming industry if cuts contained in last year’s spending review were enacted.
A reduction in the number of vets “would have a significant impact on the meat industry”, which cannot put products ranging from sausages to lamb cutlets on the market without veterinary signoff.
While efforts have been made in some sectors such as fishing to centralise the burden of red tape, the report found that, 21 months on, a shortage of vets was still affecting farm produce.
In autumn 2021 the FSA had to put temporary measures in place to ensure it was able to recruit enough qualified officials to deliver its expanded role, the report found.
It also noted that the Competition and Markets Authority (CMA) was “competing with the private sector to recruit and retain competition lawyers and economists while both the FSA and the Health and Safety Executive were “struggling to recruit experienced toxicologists in sufficient numbers”.
It added: “Regulators and policy departments should now identify the impact of potential cuts on regulatory risk and set out where significant changes in the regulatory model would be needed to mitigate them.”
Hillier called on the regulators to “work together on ways to address the loss of regulatory cooperation arrangements with the EU, and in six months we expect a progress report on how the arrangements set out in the trade and cooperation agreement are being taken forward”.
Development of long-term regulatory strategies post-Brexit “has been slow and the future direction remains unclear”, she said.
For example, the CMA’s subsidy advice unit, which will offer critical advice to companies working under the new trade deal, was not due to be operational before October 2022.
It will be two years before the HSE’s post-Brexit IT infrastructure and processes are completed and the FSA will not have full import checks on high-risk foods until the end of 2023.
FRIDAY 2ND SEPTEMBER 2022
My dear only son Andrew’s birthday, I can write no more words about his loss today as it hurts too much……
Andrew far left happier times with his best friends
THURSDAY 30TH JUNE 2022
The article and incident below ( reported 20th Sept 2021) below was ‘hidden’ from most people’s view, with the world weighed down with covid and its consequences. Its highlights how dangerous zoonotic disease continues to be to animals and the human food chain. How many dead dying animals infected with BSE have and are still entering the human food chain, and how many people in the decades to come will die of human mad cow disease? One cow has the ability to infect thousands of people via food or medicine. Infect pets by pet food, infect wildlife via them feasting on decaying/dying BSE cattle. Would any of the ministers cited in this report eat beef, meat, cheese, milk from this herd in Somerset of allow their families to make a meal from these cows? How many animals from this herd had already entered the food chain?
Catherina Cunnane
20/09/2021
BSE case ‘does not affect the UK’s ability to export beef to other countries’
The Animal and Plant Health Agency in the UK has confirmed a single case of classical Bovine Spongiform Encephalopathy (BSE).
The body detected the case on a farm in Somerset on Friday, September 17th, 2021.
The animal is deceased and was removed from the farm. It confirmed that further investigations continue to identify the origin of the disease.
in line with the?government’s disease prevention response plan, it has implementedprecautionary movement restrictions on the farm.
Chief Veterinary Officer Christine Middlemiss said:
“A single case of classical?BSE has been confirmed on a farm in Somerset. The animal died on-farm and was tested as part of our TSE surveillance controls.”
The department has implemented movement restrictions on the farm. “This is standard procedure until we have a clear understanding of the origin of the disease.”
“This is further proof that our surveillance system for detecting?and containing?this type of?disease is working.”
“We recognise this will be a traumatic time for the farmer. We are on hand to offer advice through this difficult period.”
The UK’s overall risk status for BSE remains at ‘controlled’, and there is no risk to food safety or public health.
A Food Standards Agency spokesperson said there are strict controls in place to protect consumers from the risk of BSE.
These include controls on animal feed and removing parts of cattle most likely to carry BSE infectivity.
The Animal and Plant Health Agency will now begin a thorough investigation of the herd, the premises, potential sources of infection. It will produce a full report on the incident “in due course”.
The UK has reported five cases of confirmed BSE since 2014.
All of these have been in animals which, as fallen stock, were not destined for the human food chain and posed no risk to the public.
In line with international commitments, the UK has informed the World Organisation for Animal Health and trading partners of the case.
“This does not affect the UK’s ability to export beef to other countries.” the statement concluded.
Brazil suspends beef exports to China over BSE cases
Meanwhile, earlier this month, we reported that Brazil suspended beef exports to China over BSE cases.
The country confirmed two cases of “atypical” BSE in two separate meat processing plants.
Brazil’s decisions to halt beef exports to China, following the discovery of two atypical BSE cases, presents a “huge opportunity” for Ireland.
That is according to IFA president, Tim Cullinan, who has called for the immediate resumption of Irish beef exports to China.
Minister McConalogue has said that regaining beef access to the Chinese market “remains a priority” for Ireland.
Department officials, through the Embassy of Ireland in Beijing, continue to “engage positively” with their Chinese counterparts with a view to re-opening market access for Irish beef.
However, the timing of that decision lies with the Chinese authorities, the DAFM stated.
SUNDAY 17TH APRIL 2022
Below are some photos of the art that Roger Hiorns curated/ developed at Goldsmith’s University show, which is a pitch for him to present a forever piece of art in central London. Roger’s art will be in ‘Memorial’ of all those who have died, past, present and unfortunately in the future of vcjd a zoonotic disease. A lethal virus that transmits from animal to humans is a direct response to climate change, profiteering by huge corporations more concerned with making money than animal, human and environmental health. 1918 flu pandemic, avian flu, Swine flu, human BSE, Covid 19 are all zoonotic diseases.
When will the next zoonotic pandemic hit the globe?
The art show at Goldsmiths University has now ended, but not the fight for justice and recognition for all those killed by zoonotic disease, Human BSE, Avian, Swine Flu, and of course Covid 19.
Some of photos that visitors can touch immerse and view

TUESDAY 25TH JANUARY 2022
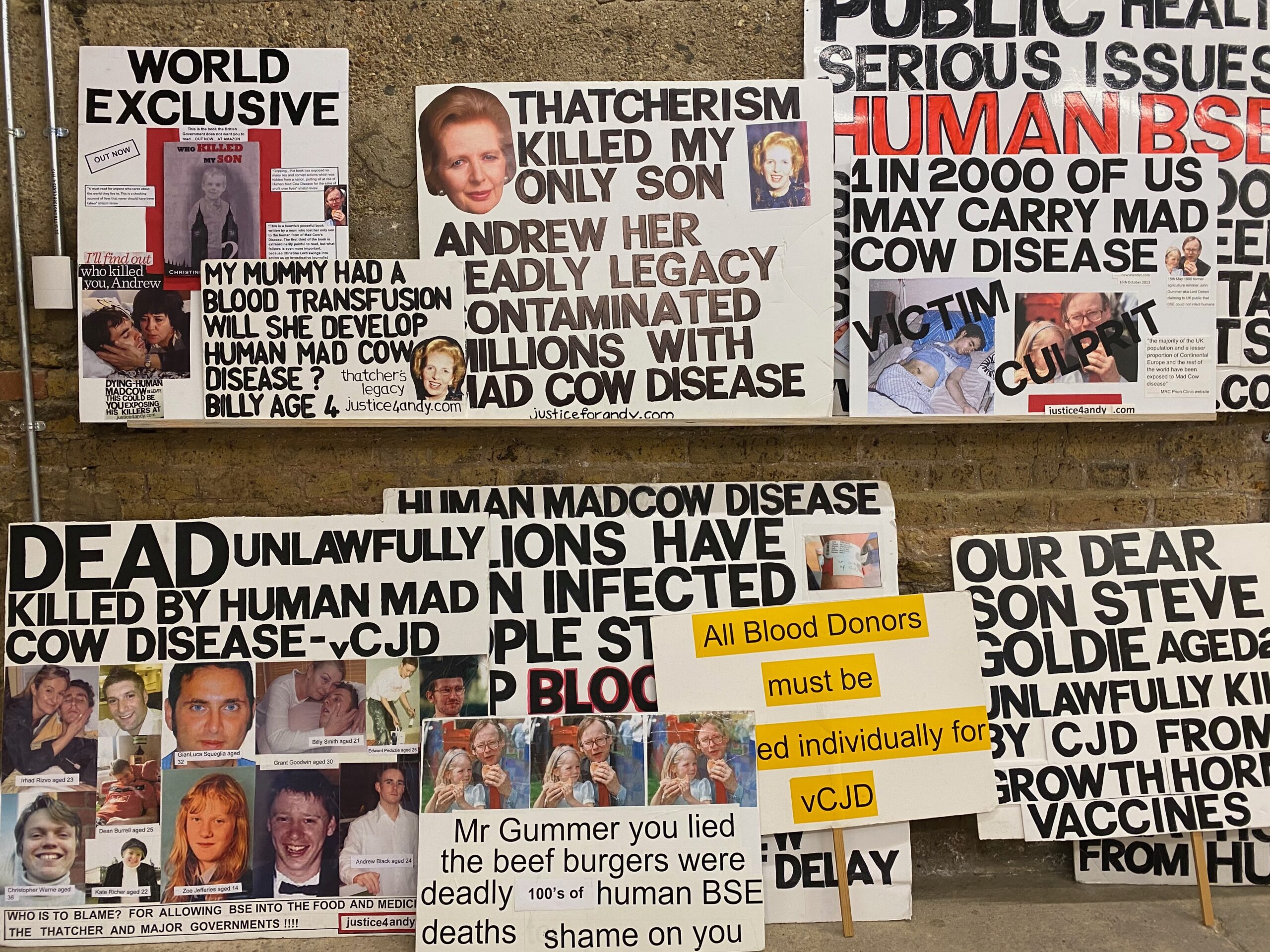
From 21st January- 3rd April 2022, a shocking art show is taking place at Goldsmiths University CAA, London using posters, photographs, research from my campaign since 2008-current. Roger Hiorns, Turner nominated artist continues to use his art and installations to highlight the importance of www.justice4andy.com campaign and it relevance to climate change, animal human health and current/future pandemics.
See the link below and some of the photos/placards/research being used as Roger’s installation. Its part of the show called ‘Testament’ which looks at the way we remember our dead and the various campaigns that have grown over reccent years. Including www.justice4andy.com. As part of the show my film ‘cows, cash and cover-ups? investigating vcjd will also be shown in its entirety.
https://goldsmithscca.art/exhibition/testament/
Some of photos that visitors can touch immerse and view
-
Investigating vCJD | Prime Video. Cows, Cash & Cover-ups? Investigating vCJD. Variant Creutzfeldt-Jakob disease (vCJD) is the human form of BSE (Mad Cow Disease) and has been described as a “ticking time bomb” by Scientists. This ground-breaking documentary explores the harrowing experiences of vCJD victims’ families.
THURSDAY 16TH DECEMBER 2021
Today on 16th December at 9.25pm in 2007, my son Andrew was killed by human BSE, the human form of mad cow disease, he was just 24 years old. BSE in humans is a zoonotic disease like Covid-19 and Avian Flu. Zoonotic diseases are lethal diseases transferred from animals to humans.
Zoonotic disease are caused by the encroachment of wildlife habitats, over farming and lack of respect for animal, human and our planets health. Deadly human pandemics are caused by big business and global governments having more interest in profit than our future generation’s lives and our planets future.
A parent never ‘gets over’ the loss of their child. Why would I ever forget my only beloved son Andrew?
The fight continues for justice for all victims of BSE and zoonotic disease including those lives needlessly lost through covid too.
I walk alongside my grief, pain and loss every second of every day. Grief and tears are about love, loss and missing and then about loving again.
During one of the last conversations I had with my son he asked me ‘ Please don’t forget me……’
I will never forget my lovely violet eyed handsome boy………

Andrew 2006
THURSDAY 2nd September 2021
Today would have been my son Andrew’s 38th birthday, but, he will be forever a young man of just 24 years old. Time does not heal when a parent loses their child. There is no resolution or peace of mind when their child has been unlawfully killed by corporate greed, political expedience, individual men and women who are and continue to be culpable and responsible for my son’s untimely death. Those same men and women who are feted, financially rewarded for their wrong doings and crimes.
There are no words for tears.
Love you always my Andrew from your Mum and sister Emma x
See you over the rainbow.
 Andrew and his little sister Emma
Andrew and his little sister Emma
SCIENCE
Émilie Jaumain in 2010, the year she was exposed to prions during a lab accident. She died in 2019 at age 33. ARMEL HOUEL
France issues moratorium on prion research after fatal brain disease strikes two lab workers
By Barbara CasassusJul. 28, 2021 , 4:35 AM
PARIS—Five public research institutions in France have imposed a 3-month moratorium on the study of prions—a class of misfolding, infectious proteins that cause fatal brain diseases—after a retired lab worker who handled prions in the past was diagnosed with Creutzfeldt-Jakob disease (CJD), the most common prion disease in humans. An investigation is underway to find out whether the patient, who worked at a lab run by the National Research Institute for Agriculture, Food and Environment (INRAE), contracted the disease on the job.
If so, it would be the second such case in France in the past few years. In June 2019, an INRAE lab worker named Émilie Jaumain died at age 33, 10 years after pricking her thumb during an experiment with prion-infected mice. Her family is now suing INRAE for manslaughter and endangering life; her illness had already led to tightened safety measures at French prion labs.
The aim of the moratorium, which affects nine labs, is to “study the possibility of a link with the [new patient’s] former professional activity and if necessary to adapt the preventative measures in force in research laboratories,” according to a joint press release issued by the five institutions yesterday.
“This is the right way to go in the circumstances,” says Ronald Melki, a structural biologist at a prion lab jointly operated by the French national research agency CNRS and the French Alternative Energies and Atomic Energy Commission (CEA). “It is always wise to ask questions about the whole working process when something goes wrong.” “The occurrence of these harsh diseases in two of our scientific colleagues clearly affects the whole prion community, which is a small ‘familial’ community of less than 1000 people worldwide,” Emmanuel Comoy, deputy director of CEA’s Unit of Prion Disorders and Related Infectious Agents, wrote in an email to Science. Although prion research already has strict safety protocols, “it necessarily reinforces the awareness of the risk linked to these infectious agents,” he says.
In Jaumain’s case, there is little doubt she was infected on the job, according to a paper published in The New England Journal of Medicine (NEJM) in 2020. She had variant CJD (vCJD), a form typically caused by eating beef contaminated with bovine spongiform encephalopathy (BSE), or mad cow disease. But Europe’s BSE outbreak ended after 2000 and vCJD virtually disappeared; the chance that someone of Jaumain’s age in France would contract food-borne vCJD is “negligible or non-existent,” according to the paper.
A scientist with inside knowledge says the new patient, a woman who worked at INRAE’s Host-Pathogen Interactions and Immunity group in Toulouse, is still alive. French authorities were apparently alerted to her diagnosis late last week. The press release suggests it’s not yet clear whether the new case is vCJD or “classic” CJD, which is not known to be caused by prions from animals. Classic CJD strikes an estimated one person per million. Some 80% of cases are sporadic, meaning they have no known cause, but others are genetic or contracted from infected human tissues during transplantations. The two types of CJD can only be distinguished through a postmortem examination of brain tissue.
Lab infections are known to occur with many pathogens, but exposure to CJD-causing prions is unusually risky because there are no vaccines or treatments and the condition is universally fatal. And whereas most infections reveal themselves within days or weeks, CJD’s average incubation period is about 10 years.
For Jaumain, who worked at INRAE’s Molecular Virology and Immunology Unit in Jouy-en-Josas, outside Paris, that long period of uncertainty began on 31 May 2010, when she stabbed her left thumb with a curved forceps while cleaning a cryostat—a machine that can cut tissues at very low temperatures—that she used to slice brain sections from transgenic mice infected with a sheep-adapted form of BSE. She pierced two layers of latex gloves and drew blood. “Émilie started worrying about the accident as soon as it had happened, and mentioned it to every doctor she saw,” says her widower, Armel Houel.
In November 2017, Jaumain developed a burning pain in her right shoulder and neck that worsened and spread to the right half of her body over the following 6 months, according to the NEJM paper. In January 2019, she became depressed and anxious, suffering memory impairment and hallucinations. “It was a descent into hell,” Houel says. She was diagnosed with “probable vCJD” in mid-March of that year and died 3 months later. A post-mortem confirmed the diagnosis.
The occurrence of these harsh diseases in two of our scientific colleagues clearly affects the whole prion community.
Emmanuel Comoy, French Alternative Energies and Atomic Energy Commission
INRAE only recently admitted the likely link between Jaumain’s illness and the accident. “We recognize, without ambiguity, the hypothesis of a correlation between Emilie Jaumain-Houel’s accident … and her infection with vCJD,” INRAE chair and CEO Philippe Mauguin wrote in a 24 June letter to an association created by friends and colleagues to publicize Jaumain’s case and lobby for improvements in lab safety. (Science has obtained a copy of the letter, which has not been made public.)
Jaumain’s family has filed both criminal charges and an administrative suit against INRAE, alleging a range of problems at Jaumain’s lab. She had not been trained in handling dangerous prions or responding to accidents and did not wear both metal mesh and surgical gloves, as she was supposed to, says Julien Bensimhon, the family’s lawyer. The thumb should have been soaked in a bleach solution immediately, which did not happen, Bensimhon adds.
Independent reports by a company specializing in occupational safety and by government inspectors have found no safety violations at the lab; one of them said there was a “strong culture” of risk management. (Bensimhon calls the reports “biased.”)
The government inspectors’ report concluded that Jaumain’s accident was not unique, however. There had been at least 17 accidents among the 100 or so scientists and technicians in France working with prions in the previous decade, five of whom stabbed or cut themselves with contaminated syringes or blades. Another technician at the same lab had a fingerprick accident with prions in 2005, but has not developed vCJD symptoms so far, Bensimhon says. “It is shocking that no precautionary measures were taken then to ensure such an accident never happened again,” he says.
In Italy, too, the last person to die of vCJD, in 2016, was a lab worker with exposure to prion-infected brain tissue, according to last year’s NEJM paper, although an investigation did not find evidence of a lab accident. That patient and the lab they worked at have not been identified.
After Jaumain’s diagnosis, “We contacted all the research prion labs in France to suggest they check their safety procedures and remind staff about the importance of respecting them,” says Stéphane Haïk, a neuroscientist at the Paris Brain Institute at Pitié-Salpêtrière Hospital who helped diagnose Jaumain and is the corresponding author on the paper. Many labs tightened procedures, according to the government inspectors’ report, for instance by introducing plastic scissors and scalpels, which are disposable and less sharp, and bite and cut-resistant gloves. A team of experts from the five research agencies is due to submit proposals for a guide to good practice in prion research to the French government at the end of this year
The scientific community has long recognized that handling prions is dangerous and an occupational risk for neuropathologists, says neuropathologist Adriano Aguzzi of the University of Zurich. Aguzzi declined to comment on the French CJD cases, but told Science his lab never handles human or bovine prions for research purposes, only for diagnostics. “We conduct research only on mouse-adapted sheep prions, which have never been shown to be infectious to humans,” Aguzzi says. In a 2011 paper, his team reported that prions can spread through aerosols, at least in mice, which “may warrant re-thinking on prion biosafety guidelines in research and diagnostic laboratories,” they wrote. Aguzzi says he was “totally shocked” by the finding and introduced safety measures to prevent aerosol spread at his own lab, but the paper drew little attention elsewhere.
The moratorium will “obviously” cause delays in research, but given the very long incubation periods in prion diseases, the impact of a 3-month hiatus will be limited, Comoy says. His research team at CEA also works on other neurodegenerative diseases, including Alzheimer’s disease and Parkinson’s disease, and will shift some of its efforts to those.
Although Jaumain’s diagnosis upset many in the field, it hasn’t led to an exodus among researchers in France, Haïk says: “I know of only one person who resigned because they were so worried.”
With reporting by Martin Enserink.
Posted in: EuropeHealthScientific Community
doi:10.1126/science.abl658
FRIDAY JUNE 11th 2021
There has been a plaque for BSE victims for decades outside of St Thomas’ Hospital, London, UK. It is so small, families could not afford a bigger stone, often people just walked past. Now with 150 thousand hearts painted in memory of UK covid victims surrounding the BSE plaque, finally, my son Andrew and all victims of zoonotic disease, Covid and BSE are getting the publicity they need and deserve. Now all victims of zoonotic disease, Human BSE, Covid-19 need the justice and truth that the UK government have been hiding for so long!

Heart Wall and BSE memorial Plague outside St Thomas’ Hospital, London.
MONDAY 29TH MARCH 2021
The recent article in the Mirror newspaper online (below) and many other leading media outlets, investigate the 16 deadly diseases that may well be the next pandemic, which could ‘devastate civilisation.’
On the list is Human BSE, vCJD Human form of mad cow disease. Human BSE has an incubation period in humans upwards 50 years and 1 in 2,000 of the UK population are carrying or incubating Human BSE with the ability to pass it onwards through medical proceedures. These articles report on, ‘The Coalition for Epidemic Preparedness Innovations (CEPI)’, an organisation founded by the Bill and Melinda Gates Foundation, Wellcome Trust and several nations.
DAILY MIRROR 22nd March 2021
https://www.mirror.co.uk/news/world-news/16-diseases-eyebleeding-fever-explosive-23776174
16 diseases from eye bleeding fever to explosive diarrhoea that could be the next Covid
The Coalition for Epidemic Preparedness Innovations (CEPI), an organisation founded by the Bill and Melinda Gates Foundation, the Wellcome Trust, and several nations, has published the list of diseases
Diseases which could “shatter” civilisation if they were to begin spreading have been identified in a new report.
The 16 illnesses have emerged in countries across the world and have the potential to trigger a new pandemic, it has been claimed.
While some are well known to those in the West, such as E. coli and HIV, others are less known but just as deadly, with one causing bleeding from orifices and another brain swelling.
The diseases have been highlighted in a report published by the Coalition for Epidemic Preparedness Innovations (CEPI), an organisation founded by the Bill and Melinda Gates Foundation, the Wellcome Trust, and several nations.
The document warns: “Covid-19 is just one of many diseases with pandemic potential.
“More than 1.6 million yet to be discovered viral species from these virus families are thought to exist in mammal and bird hosts.
“And any of these could be the next Covid, or worse.”
Highlighted in the report are coronaviruses other than Covid-19, which could rip through the world’s populations with even deadlier consequences.
It warns: “The emergence of a coronavirus combining the transmissibility of Covid-19 with the lethality of SARS or MERS would be civilisation-shattering.”
Future pandemics could prove deadlier than coronavirus, the organisation warned
Other diseases could make a deadly comeback, according to CEPI, such as HIV and Ebola in Africa.
One of the conditions on the list shares similar qualities to the Bubonic Plague, which was passed to humans from the fleas on rats
Lassa fever is passed from rodents to rats and can result in facial swelling, bleeding from the mouth, nose, eyes and vagina, and seizures in severe cases.
Last year the condition, which leads to a quarter of surviving patients temporarily losing their hearing, claimed 144 lives in Nigeria and has a fatality rate of about 1 in 100.
Currently there is no known cure or vaccine, with isolating patients, staying away from Rodent droppings and getting a cat the best hope people have.
Many of the diseases on the list have no or not particularly effective cures
Another lesser known disease, Cryptosporidiosis, has already had a minor outbreak in the UK.
The diarrhoea disease, which is caused by microscopic parasites, lives in the intestines of humans and animals but can survive outside the body for long periods of time, including in swimming pools and hot tubs.
16 diseases which could cause the next pandemic
E.coli 0157:H7 – A bacteria found in food, often in milk and ground beef
Cyclosporiasis – An intestinal illness caused by eating food contaminated with parasite
Whitewater arroyo virus – Viral infection found in wood rats that can cause liver failure
Hantavirus pulmonary syndrome – A respiratory disease carried by rats which kills a third of patients
HIV – A virus attacking the body’s immune system which can lead to AIDS, an auto-immune disease
Nipah – This disease causes severe brain swelling, seizures and vomiting
Hendra virus – Passed from flying-foxes to horses and then to humans, it has a 70% fatality rate
Ebola – A viral fever which can lead to red eyes and unexplained bleeding
Marburg – A viral hemorrhagic fever in the same family as Ebola
Hepatitis C – A blood borne illness which can cause liver cancer
Lassa fever – A potentially fatal condition which causes facial swelling, bleeding from the mouth, nose and vagina
SARS – An airborne coronavirus which spreads in a similar way to flu that has been eradicated in humans, but could be passed back through animals again
Cryptosporidiosis – A diarrheal disease that can live in the intestines of humans and animals as well as in warm water
vCJD – A brain disease passed on through eating infected beef which can cause psychiatric problems, behavioural changes, and painful sensations.
H5NI Influenza – A highly infectious strain of bird flu which attacks the respiratory system
Enterovirus 71 – A neurological disease which can cause hand, foot and mouth disease in children
A cluster of cases of the disease, which can be particularly harmful to children, was seen in the West Midlands in 2016.
If it is left untreated in patients with weakened immune systems it can become chronic and even fatal.
Another disease to watch out for is Nipah, which is bat-borne and has had outbreaks in South-East and South Asia.
The neurological disease causes severe brain swelling, seizures and vomiting and has a fatality rate as high as 70%.
Other fatal diseases include Whitewater Arroyo virus which was thought not to be able to pass to humans until it killed three women in California, including a 14-year-old girl.

Andrew as a baby
WEDNESDAY 24th FEBRUARY 2021
I have recently received my vaccine, to prevent me from becoming seriously ill with covid-19, with little discomfort or side effects. I decided to have the vaccine after making an informed choice. Unlike the 1980s, 1990s, and early 2000’s when vaccines were sourced from BSE cattle, their production and ingredients kept secret. Everything possible has been public about how the current vaccines to prevent covid-19 have been produced. I took the vaccine as I wanted to protect myself, my community. We have a collective responsibility to protect each other. Vaccination seems the only way forward. This will prevent hundreds of thousands more avoidable deaths, allowing covid-19 to mutate into a virus similar to winter cold/flu, manageable by vaccination or medications
BSE was the harbinger of Covid, both avoidable zoonotic diseases that came from an animal and transferred to humans. Both created by lack of respect for our planet, animal and human health. If the UK and world governments do not take heed, we as a global community could face a series of other deadly zoonotic disease. Our lives, and future generations lives never reverting to the freedoms of movement we had before 2020.
This is not a world I want to live in….so we must all think about the future, our planet and each other and protect them.
I wish there had been a vaccine to prevent BSE in cattle and vcjd, in humans, I wish BSE had never been created.
I wish my son Andrew was still here with me and his family.
SATURDAY 23RD JANUARY 2021
The biggest vaccination programme in the UK’s history is taking place, as people are called to have the vaccine. This will hopefully help prevent millions of people becoming seriously ill with covid-19. Another deadly zoonotic disease, first recognised in China which originated in bats and then transferred to humans. Covid-19 transmits via coughs, sneezes and close contact with other people, a lethal flu that is new and therefore our immune systems are unable to cope. Millions across the world have died and 100,00 people in the UK. This pandemic must be controlled and at present the only way forward is vaccination.
I have thoroughly researched the vaccines and ingredients, and with an informed mind I will be having the vaccine when I am able. The covid-19 immunisation programme has been overseen by scientists, experts, media and the public.
FRIDAY JANUARY 22ND 2021
With the lowering of UK safety standards regarding food imports, (see Guardian article below) it will mean zoonotic disease such as BSE, Avian flu, will have easier access to the UK and its residents. It could result in the next pandemic.
Once again these ‘Trade Bills’ post BREXIT are about economics and making a ‘fast buck’ with big foreign corporations for shareholders, political gain and with human and animal health bottom of the list. With Chronic Wasting Disease CWD, the equivalent of BSE in deer, cervids, elks rampaging across the USA and parts of Canada, its mean this disease could be imported into the UK. There are many cases of deer hunters and people associated with deer developing dementia type disease similar to cjd.
UK ministers gain power to allow lower-standard food imports
Trade bill vote rejects Lords amendment giving MPs greater scrutiny of trade deals
A chicken processing plant in the US.
A chicken processing plant in the US. Photograph: Glowimages/Getty
Fiona Harvey Environment correspondent
Tue 19 Jan 2021 20.06 GMT
5,139
Ministers will be able to approve the import of animal and agricultural products of a lower standard than currently permitted in the UK, after attempts to amend the trade bill failed.
The government has repeatedly vowed not to allow the import of chlorinated chicken and hormone-treated beef, but has refused to sign those pledges into law.
The House of Lords put forward amendments to the trade bill that would have required future trade agreements to be scrutinised by parliament, with a view to ensuring standards are retained, but the key amendment fell on Tuesday night by 353 votes to 277.
Campaigners said the new post-Brexit arrangements for food imports and food production standards in the UK would allow ministers to make sweeping changes to existing food safety regulations without consultation.
Advertisement
Many products could be affected. For instance, while the government has said it will not allow chlorinated chicken, meat can be washed in a variety of other substances that have similar effects: peracetic acid, cetylpyridinium chloride, acidified sodium chlorite, or organic acid rinses.
Chicken treated with bleach and similar substances can retain some pathogens, according to research, and campaigners also fear that such treatment is used to disguise infections caused by animals being kept in poor conditions that would be illegal in this country.
In the debate, the government sought to reassure MPs that there were sufficient safeguards to ensure the UK’s standards were kept high.
However, there was disagreement. Jonathan Djanogly, one of a small number of Conservative MPs who voted against the government, said: “Ministers suggest that a pre-signature vote [on a trade deal] would make them look less decisive and weaken their hand, but I would suggest that the opposite is actually the case. In the US, negotiations are often strengthened by the executive suggesting that Congress won’t accept such-and-such a proposal.”
He added: “The power of approval that was given to MEPs now needs to come back here to parliament, not to be forgotten by ministers. Having proper scrutiny votes will go towards establishing the UK as a modern, democratic, confident, international trading nation, and we should be embracing that.”
Campaigners pointed to loopholes in the government’s regulations that mean food standards can be altered without consultation or fanfare. They said the rules would make it difficult to even find out whether standards had been lowered.
For instance, the list of approved antibiotics for livestock – a vital issue, because the overuse of antibiotics on livestock is a key driver of the growth of antibiotic resistance that threatens human medicine – can be changed without notice, and only close retrospective scrutiny would reveal the changes.
Kierra Box, a campaigner at Friends of the Earth, said: “MPs have voted to lock themselves out of decisions on future trade deals. These deals will have a far bigger impact than changing the contents of our supermarket shelves. They could make it harder to pass new legislation to protect our environment, increase the UK’s contribution to climate change, or prop up supply chains linked to human rights abuses. It’s not just disappointing that our elected representatives are willing to let themselves and their constituents be satisfied – it’s mystifying.”
Debbie Tripley, the director of environmental policy and advocacy at WWF-UK, said: “The government’s approach to trade risks undermining their ambition to be a global green leader. Ministers should not have powers to remove important protections via loophole, nor push future trade deals through parliament without meaningful scrutiny.”
Recent research suggests the government may run into trouble with its “red wall” voters if food standards are lowered in trade deals. Qualitative research among focus groups of 52 first-time Conservative voters in red wall constituencies, carried out by Unchecked UK in partnership with KSBR Brand Futures, found strong support for stringent food standards.
Friday 22nd January 2021
With the lowering of UK safety standards regarding food imports, (see Guardian article below) t will mean zoonotic disease such as BSE, Avian flu, will have easier access to the UK and its residents. It could result in the next pandemic.
Onceain these ‘Trade Bills’ post BREXIT are about economics and making a ‘fast buck’ with big foreign corporations for shareholders, political gain and with human and animal health bottom of the list. With Chronic Wasting Disease CWD, the equivalent of BSE in deer, cervids, elks rampaging across the USA and parts of Canada, its mean this disease could be imported into the UK. There are many cases of deer hunters and people associated with deer developing dementia type disease similar to cjd.
UK ministers gain power to allow lower-standard food imports
Trade bill vote rejects Lords amendment giving MPs greater scrutiny of trade deals
A chicken processing plant in the US.
A chicken processing plant in the US. Photograph: Glowimages/Getty
Fiona Harvey Environment correspondent
Tue 19 Jan 2021 20.06 GMT
5,139
Ministers will be able to approve the import of animal and agricultural products of a lower standard than currently permitted in the UK, after attempts to amend the trade bill failed.
The government has repeatedly vowed not to allow the import of chlorinated chicken and hormone-treated beef, but has refused to sign those pledges into law.
The House of Lords put forward amendments to the trade bill that would have required future trade agreements to be scrutinised by parliament, with a view to ensuring standards are retained, but the key amendment fell on Tuesday night by 353 votes to 277.
Campaigners said the new post-Brexit arrangements for food imports and food production standards in the UK would allow ministers to make sweeping changes to existing food safety regulations without consultation.
Advertisement
Many products could be affected. For instance, while the government has said it will not allow chlorinated chicken, meat can be washed in a variety of other substances that have similar effects: peracetic acid, cetylpyridinium chloride, acidified sodium chlorite, or organic acid rinses.
Chicken treated with bleach and similar substances can retain some pathogens, according to research, and campaigners also fear that such treatment is used to disguise infections caused by animals being kept in poor conditions that would be illegal in this country.
In the debate, the government sought to reassure MPs that there were sufficient safeguards to ensure the UK’s standards were kept high.
However, there was disagreement. Jonathan Djanogly, one of a small number of Conservative MPs who voted against the government, said: “Ministers suggest that a pre-signature vote [on a trade deal] would make them look less decisive and weaken their hand, but I would suggest that the opposite is actually the case. In the US, negotiations are often strengthened by the executive suggesting that Congress won’t accept such-and-such a proposal.”
He added: “The power of approval that was given to MEPs now needs to come back here to parliament, not to be forgotten by ministers. Having proper scrutiny votes will go towards establishing the UK as a modern, democratic, confident, international trading nation, and we should be embracing that.”
Campaigners pointed to loopholes in the government’s regulations that mean food standards can be altered without consultation or fanfare. They said the rules would make it difficult to even find out whether standards had been lowered.
For instance, the list of approved antibiotics for livestock – a vital issue, because the overuse of antibiotics on livestock is a key driver of the growth of antibiotic resistance that threatens human medicine – can be changed without notice, and only close retrospective scrutiny would reveal the changes.
Kierra Box, a campaigner at Friends of the Earth, said: “MPs have voted to lock themselves out of decisions on future trade deals. These deals will have a far bigger impact than changing the contents of our supermarket shelves. They could make it harder to pass new legislation to protect our environment, increase the UK’s contribution to climate change, or prop up supply chains linked to human rights
FRIDAY 22ND JANUARY 2021
With the lowering of UK safety standards regarding food imports, (see Guardian article below) it will mean zoonotic disease such as BSE, Avian flu, will have easier access to the UK and its residents. It could result in the next pandemic.
Once again these ‘Trade Bills’ post BREXIT are about economics and making a ‘fast buck’ with big foreign corporations for shareholders, political gain and with human and animal health bottom of the list. With Chronic Wasting Disease CWD, the equivalent of BSE in deer, cervids, elks rampaging across the USA and parts of Canada, its mean this disease could be imported into the UK. There are many cases of deer hunters and people associated with deer developing dementia type disease similar to cjd.
THE GUARDIAN
UK ministers gain power to allow lower-standard food imports
Trade bill vote rejects Lords amendment giving MPs greater scrutiny of trade deals
Fiona Harvey Environment correspondent
Tue 19 Jan 2021 20.06 GMT
Ministers will be able to approve the import of animal and agricultural products of a lower standard than currently permitted in the UK, after attempts to amend the trade bill failed.
The government has repeatedly vowed not to allow the import of chlorinated chicken and hormone-treated beef, but has refused to sign those pledges into law.
The House of Lords put forward amendments to the trade bill that would have required future trade agreements to be scrutinised by parliament, with a view to ensuring standards are retained, but the key amendment fell on Tuesday night by 353 votes to 277.
Campaigners said the new post-Brexit arrangements for food imports and food production standards in the UK would allow ministers to make sweeping changes to existing food safety regulations without consultation.
Many products could be affected. For instance, while the government has said it will not allow chlorinated chicken, meat can be washed in a variety of other substances that have similar effects: peracetic acid, cetylpyridinium chloride, acidified sodium chlorite, or organic acid rinses.
Chicken treated with bleach and similar substances can retain some pathogens, according to research, and campaigners also fear that such treatment is used to disguise infections caused by animals being kept in poor conditions that would be illegal in this country.
In the debate, the government sought to reassure MPs that there were sufficient safeguards to ensure the UK’s standards were kept high.
However, there was disagreement. Jonathan Djanogly, one of a small number of Conservative MPs who voted against the government, said: “Ministers suggest that a pre-signature vote [on a trade deal] would make them look less decisive and weaken their hand, but I would suggest that the opposite is actually the case. In the US, negotiations are often strengthened by the executive suggesting that Congress won’t accept such-and-such a proposal.”
He added: “The power of approval that was given to MEPs now needs to come back here to parliament, not to be forgotten by ministers. Having proper scrutiny votes will go towards establishing the UK as a modern, democratic, confident, international trading nation, and we should be embracing that.”
Campaigners pointed to loopholes in the government’s regulations that mean food standards can be altered without consultation or fanfare. They said the rules would make it difficult to even find out whether standards had been lowered.
For instance, the list of approved antibiotics for livestock – a vital issue, because the overuse of antibiotics on livestock is a key driver of the growth of antibiotic resistance that threatens human medicine – can be changed without notice, and only close retrospective scrutiny would reveal the changes.
Kierra Box, a campaigner at Friends of the Earth, said: “MPs have voted to lock themselves out of decisions on future trade deals. These deals will have a far bigger impact than changing the contents of our supermarket shelves. They could make it harder to pass new legislation to protect our environment, increase the UK’s contribution to climate change, or prop up supply chains linked to human rights abuses. It’s not just disappointing that our elected representatives are willing to let themselves and their constituents be satisfied – it’s mystifying.”
Debbie Tripley, the director of environmental policy and advocacy at WWF-UK, said: “The government’s approach to trade risks undermining their ambition to be a global green leader. Ministers should not have powers to remove important protections via loophole, nor push future trade deals through parliament without meaningful scrutiny.”
Recent research suggests the government may run into trouble with its “red wall” voters if food standards are lowered in trade deals. Qualitative research among focus groups of 52 first-time Conservative voters in red wall constituencies, carried out by Unchecked UK in partnership with KSBR Brand Futures, found strong support for stringent food standards.
WEDNESDAY 16TH DECEMBER 2020
On this day 16th December 2007 my beloved boy Andrew who was just 24 years old, was unlawfully killed by the human form of mad cow disease, Human BSE, vCJD, prion disease. A zoonotic disease, transferred from animals to humans, like covid 19, totally avoidable. My son was killed at the altar of shareholders greed, government agendas/policies, and the disregard for human and animal health, profit paramount. As we end 2020 and still face a global pandemic due to another zoonotic and avoidable disease covid and with a vaccine against the coronavirus on the horizon. Please let’s hope lessons have been learnt. So that the world our children and children’s, children inherit do not face a life of cyclical pandemics, death, destruction and isolation. We must address the way we farm, the way government allow food to be manufactured and processed. Our global food systems are not sustainable, safe or useful. If this is not addressed then life will never return to normal or any of us globally have the freedoms we once enjoyed pre 2020.

MONDAY 19TH OCTOBER 2020
I was interviewed by presenter Ian Collins on TalkRADIO. My son Andrew worked with Ian at TalkRADIO producing many shows before he died in 2007. Ian and I discuss the latest scandal of the House of Commons stripping out an amendment which the House of Lords had included in the Agriculture Bill. This now means that imported food can have much lower safety standards, post BREXIT. Standards which would be illegal in the UK. A crisis awaiting the next pandemic?
https://www.youtube.com/watch?v=IsjnHC-fz2E&ab_channel=MadCowDiseaseVideos3
https://www.youtube.com/watch?v=IsjnHC-fz2E&ab_channel=MadCowDiseaseVideos3
MONDAY 5TH OCTOBER 2020
PORTSMOUTH NEWS UK
https://www.portsmouth.co.uk/health/southsea-investigative-journalist-says-animal-health-government-cutbacks-next-pandemic-waiting-happen-2974338
Southsea investigative journalist says animal health government cutbacks is ‘next pandemic waiting to happen’
AN INVESTIGATIVE journalist who has spent her career researching and uncovering stories on animal diseases after her son died from of mad cow disease says government cutbacks on animal health means the ‘next pandemic is waiting to happen’.
By Millie Salkeld
Wednesday, 16th September 2020, 6:22 pm
Christine Lord from Southsea was left devastated when vCJD (Creutzfeldt-Jakob Disease), the human form of mad cow disease, killed her only son Andrew Black, when he was just 24, back in December 2007
Since she has investigated the origins and spread of zoonotic diseases, animal diseases that transfer to humans, and last year was an associate producer on Cows, Cash & Cover-ups? Investigating vCJD (Creutzfeldt-Jakob Disease), which explored calls for a criminal inquiry to be held to examine the handling of the BSE crisis by the government and authorities in the farming and food industries.

Christine and Andrew xmas New York, Central Park
Christine said: ‘Zoonotic diseases, animal diseases that transfer to humans are avoidable, and as a journalist I have been investigating their origins and the way they are enabled by government policy for over a decade.
‘In 2018 the World Health Organisation published a paper on the prevention of pandemics they said one of the risk factors was intensive farming. The report stated that emerging viruses were mostly zoonotic diseases. Animal disease transferred to humans includes BSE, Swine Flu, Avian flu and of course Covid-19.

Chrisitne filming with BBC1 Countryfile
‘The more cattle, farmed animals that are squashed together in smaller spaces on large farms with most of the animals genetically similar and encroaching on wildlife habitats, the more likely there will be new zoonotic diseases.’
Christine featured on BBC1’s Countryfile last week to talk to presenter Tom Heap about zoonotic diseases
‘Food has become a product driven by big business and shareholders profits, when food for our families should be nourishing, sustainable and most importantly safe.
‘christine interview countryfile 13th September 2020 zoonotic diseaseWe must respect animal health and wellbeing, human health, our environment and planet otherwise I fear we may have regular and global cycles of social and economic lockdown due to emerging and preventable animal diseases.
‘This is not a legacy I want for now or for future generations.’
SUNDAY 13TH SEPTEMBER 2020
I have been filming with BBC1 Countryfile and the TV package broadcast this evening at 6pm, see below. I discuss zoonotic diseases, animal diseases that have transferred to humans. Zoonotic disease include BSE, Avian Flu, Swine Flu and of course Covid-19. I talk about emerging diseases, government cutbacks, encroachment of wildlife and a developing crisis awaiting the next pandemic?
WEDNESDAY 2nd September 2020
Today would have been my only son Andrew’s birthday. As the years pass I miss him more, not less. The conversations never said, the laughs never heard, the hugs never received. The days, week, months and now years that were unlawfully taken from my Andrew.
Love always to my son on this his birthday, still missing you so much.
Mumx

FRIDAY 31ST JULY 2020
The same calming rhetoric used to disguise and hide the dangers of BSE now being used during the Covid-19 pandemic? See this timely newspaper report below. What does the ‘best scientific advice’ mean? Is it meaningless when its manipulated by civil servants and politicians to fit policy!?
THE GUARDIAN
https://www.theguardian.com/commentisfree/2020/jul/23/bias-science-bse-coronavirus-crisis
Bias in ‘the science’ on coronavirus? Britain has been here before
Lessons about scientific transparency from the BSE scandal have been forgotten as the government grapples this crisis
Last modified on Fri 24 Jul 2020 21.17 BST
It became the defining moment of the BSE crisis. In an attempt to persuade the public that it was perfectly safe to eat beef, the then agriculture minister, John Gummer, fed his four-year-old daughter a burger on camera in 1990. Six years later, the government admitted there was a link between eating infected beef and the brain disease vCJD, though thankfully the numbers affected were relatively small. Nevertheless, the scandal eroded public trust in government public health messaging, with knock-on effects on parents’ perception of government advice during the MMR scandal, a few years later.
The Gummer moment should serve as a warning to politicians about what happens if they seek to patronise the public with assurances that are not backed up by science. Yet there are already several candidates for the coronavirus equivalent. Will it be Boris Johnson boasting of “shaking hands with everybody” on 3 March? His claim on 12 March that banning large events would have little effect? Or his assurances that the government will avoid another national lockdown?
The public inquiry into the BSE scandal resulted in a 16-volume report that called for greater transparency in the production and use of scientific advice, and for the public to be treated like grownups who can understand uncertainty. Twenty years later, those lessons appear to have been forgotten.
One of the questions already being asked is why the government took so long to implement a full lockdown. There were two narratives that emerged from the government’s science advisers in the early days: that it would be wrong to suppress the spread of Covid-19 altogether as this would prevent “herd immunity” building up, and that the public would only tolerate a lockdown for so long. In a programme for Radio 4 this week, I looked at where this pseudo-scientific idea of “behavioural fatigue” came from: none of the behavioural scientists I interviewed – including those who sit on Sage’s behavioural science subcommittee – knew. Similar questions remain about exactly how the idea of pursuing herd immunity emerged.
One thing is clear. The government’s science advisers are repeating the mistakes of the BSE crisis – confusing a lack of evidence of risk or benefit for a lack of risk or benefit altogether. The deputy chief medical officer, Jenny Harries, asserted back in March that mask wearing was “not a good idea” for members of the public because it could increase the risk of contracting the virus. The developing evidence base on masks contradicts this. Others have made the same error: the World Health Organization has for months insisted that Covid-19 is transmitted through droplets when people cough or sneeze, rather than through much finer aerosols that can linger in the air for longer. But there was little certainty around this, and new evidence suggests that aerosol transmission may indeed be an issue.
At the root of all this is the nature of scientific knowledge. It is rarely black and white, and this is never truer than with a new disease, what the science historian Lorraine Daston has dubbed an “empirical ground zero”. That ground zero entails a high degree of uncertainty, which paves the way for human bias. The paradox of science is that it is that while it aspires to peeling away bias to leave knowledge that is pure and true, it is practised by human beings who are as subject to biases as the rest of us.
As understanding of the problem of bias in science has grown, there has been much soul-searching about how to reduce it by improving the way research gets reviewed and scrutinised. But there has been much less focus on how to eliminate bias from the production of scientific advice for government.
A brilliant scientist will not necessarily be a brilliant scientific adviser. An adviser needs to be able to communicate findings outside their area of expertise, to juggle contradictory views, and to act as a conduit between academia and high politics. And there are structural incentives towards bias in scientific advice. Politicians suffer from confirmation bias – looking for evidence that supports their worldview. Boris Johnson – a self-professed libertarian aware of the economic risks of Brexit – would hardly have been keen to shut down the economy; little wonder the flawed ideas of behavioural fatigue and herd immunity got traction. Politicians also like certainty: despite Brexiteer scepticism about experts, this government has used the mantra that it is “following the science” as a shield for its political decision making.
But scientific advisers can also be complicit. Peter Lunn, a behavioural scientist who advised the Irish government there was no evidence for behavioural fatigue, told me that in his experience, scientists tend to be more strident in communicating evidence if they know it will chime with what politicians want to hear. This is why there needs to be more transparency about the processes through which scientific advice feeds into decision making.
The role of Sage versus the role of the chief scientific adviser, at present Patrick Vallance, is too fuzzily defined. Sage was set up as an ad hoc group with a rotating cast of scientists, yet is being held collectively accountable in a way that does not reflect this status. Its minutes are now being published, but do not adequately express dissenting opinion. We know too little about how the chief scientific adviser, who chairs Sage, funnels its range of opinions into government. It would create much clearer lines of accountability if Vallance’s advice, drawing on Sage input, was published as such. But the only way to get a sense of that advice in real time has been when he stands at a Downing Street podium, a troubling politicisation of the independent scientist’s role. This is even more troubling given reports that the chief nursing officer was dropped from press conference line-ups after she refused to back Dominic Cummings over his breach of lockdown guidelines.
The lack of clarity also fails to protect scientific advisers from accusations of bias. For instance, back in March, Vallance – who says his job is to speak scientific truth to power – was seen as a favourite for the role of chief executive of UK Research and Innovation, a £7bn -a-year science funding body, an appointment that Cummings, obsessed with science policy, would have likely had influence over. This would be a tricky position for anyone to negotiate, regardless of their integrity, and greater transparency would have insulated Vallance from the accusation that it might have affected his ability to deliver difficult messages.
Certainty comes across as authoritative, even when it is anything but. It is not just the government’s advisers who fall prey to this; some of its strongest scientific critics have also downplayed uncertainty. There are those who are keen to pin 100% of the blame on the politicians, and those who would rather it was all laid at the door of their scientific advisers. But I suspect any inquiry will produce lessons eerily similar to those of the BSE report. Back then, the absence of systems to protect scientific advice from bias were partly to blame. It seems not much has changed.
- Sonia Sodha is a Guardian columnist
FRIDAY 3rd JULY 2020
A French lab technician died of vCJD in 2019, 7.5 years after she cut herself in a lab whilst handling mice infected with BSE. The woman was just 24 years old when she was infected and died when she was 31 years old. This shows how dangerous BSE is even within a bio-hazard environment.
This new research below highlights that scientists and governments are still researching BSE and its on-going consequences to humans and animals globally, and the ease with which the rogue prions that cause vcjd can be transmitted to humans. Via fluids, blood, droplets, medical proceedures and other events in which medics, scientists, care workers and those working in abattoirs and meat markets can be exposed
Variant Creutzfeldt–Jakob Disease Diagnosed 7.5 Years after Occupational Exposure
July 2nd 2020
Variant Creutzfeldt–Jakob disease was identified in a technician who had cut her thumb while handling brain sections of mice infected with adapted BSE 7.5 years earlier. The long incubation period was similar to that of the transfusion-transmitted form of the disease.
TO THE EDITOR:
We report a case of variant Creutzfeldt–Jakob disease (CJD) that was plausibly related to accidental occupational exposure in a technician who had handled murine samples contaminated with the agent that causes bovine spongiform encephalopathy (BSE) 7.5 years earlier.
In May 2010, when the patient was 24 years of age, she worked in a prion research laboratory, where she handled frozen sections of brain of transgenic mice that overexpressed the human prion protein with methionine at codon 129. The mice had been infected with a sheep-adapted form of BSE. During this process, she stabbed her thumb through a double pair of latex gloves with the sharp ends of a curved forceps used to handle the samples. Bleeding was noted at the puncture site.
In November 2017, she began having burning pain in the right shoulder and neck. The pain worsened and spread to the right half of her body during the following 6 months. In November 2018, an examination of a sample of cerebrospinal fluid (CSF) obtained from the patient was normal. Magnetic resonance imaging (MRI) of the brain showed a slight increase in the fluid-attenuated inversion recovery (FLAIR) signal in the caudates and thalami (Fig. S1A and S1B in the Supplementary Appendix, available with the full text of this letter at NEJM.org). In January 2019, she became depressed and anxious and had memory impairment and visual hallucinations. There was hypertonia on the right side of her body. At that time, an analysis of CSF for 14-3-3 protein was negative. In March 2019, MRI showed an increased FLAIR signal in pulvinar and dorsomedial nuclei of thalami (Fig. S1C through S1E).
The patient was found to be homozygous for methionine at codon 129 of the prion protein gene without mutation. An analysis of a sample of CSF on real-time quaking-induced conversion analysis was negative for a diagnosis of sporadic CJD. However, an analysis of plasma and CSF by means of protein misfolding cyclic amplification was positive for the diagnosis of variant CJD (Figure 1A and 1B). The patient died 19 months after the onset of symptoms. Neuropathological examination confirmed the diagnosis of variant CJD (Figure 1C and 1D). Western blot analysis showed the presence of type 2B protease-resistant prion protein in all sampled brain areas. The clinical characteristics of the patient and the postmortem neuropathological features were similar to those observed in 27 patients with variant CJD who had previously been reported in France.1 (Additional details are provided in the Supplementary Appendix.)
There are two potential explanations for this patient’s condition. Oral transmission from contaminated cattle products cannot be ruled out because the patient was born at the beginning of the French BSE outbreak in cattle. However, the last two patients who had confirmed variant CJD with methionine homozygosity at codon 129 in France and the United Kingdom died in 2014 and 2013, respectively, which makes oral transmission unlikely. In France, the risk of variant CJD in 2019 was negligible or nonexistent in the post-1969 birth cohort.
Percutaneous exposure to prion-contaminated material is plausible in this patient, since the prion strain that she had handled was consistent with the development of variant CJD.3 The 7.5-year delay between the laboratory accident and her clinical symptoms is congruent with the incubation period in the transfusion-transmitted form of the disease. The ability of this strain to propagate through the peripheral route has been documented, and experimental studies with scrapie strains have shown that scarification and subcutaneous inoculation are effective routes.4,5 The last known Italian patient with variant CJD, who died in 2016, had had occupational contact with BSE-infected brain tissues, although subsequent investigation did not disclose a laboratory accident (Pocchiari M, Italian Registry of CJD: personal communication). Thus, the last two cases of variant CJD outside the United Kingdom have been associated with potential occupational exposure. Such cases highlight the need for improvements in the prevention of transmission of variant CJD and other prions that can affect humans in the laboratory and neurosurgery settings, as outlined in the Supplementary Appendix
Jean-Philippe Brandel, M.D. Assistance Publique–Hôpitaux de Paris, Paris, Franc
- Bustuchina Vlaicu, M.D. Groupe Hospitalier Nord-Essonne, Orsay, Franc
Audrey Culeux, B.Sc. INSERM Unité 1127, Paris, Franc
Maxime Belondrade, M.Sc. Daisy Bougard, Ph.D. Etablissement Français du Sang, Montpellier, Franc
Grznarova, Ph.D. Angeline De
TUESDAY 16th JUNE 2020
THIS IS HOW THE UK CONSERVATIVE GOVERNMENT IS ACTING DURING THE CORONAVIRUS EMERGENCY TO SECURE A TRADE DEAL WITH TRUMP.
SE SKY NEWS REPORT BELOW.
BREXIT IS LOOMING AT THE END OF THIS YEAR AND TRUMP KNOWS BORIS JOHNSON AND HIS GOVT ARE LOOKING TO MAKE AS MUCH MONEY AS POSSIBLE,UK PUBLIC HEALTH AND SAFETY AT THE BOTTOM OF THE LIST.

Christine with Len MCluskey Gen Sec UNITE Labour Conference, Brighton, UK.
NEXT THE NHS WILL BE ON THE TABLE!
SKY NEWS
US trade deal ‘could pose greatest risk to UK food since BSE crisis’
https://apple.news/AKeAbFa4ATFKOYSAydNxTgA
BSE killed my son. Mad cow disease & Covid-19 zoonotic diseases. 95 million US cattle just 10 thousand tested yearly for BSE
US trade deal ‘could pose greatest risk to UK food since BSE crisis’
Consumer group Which? is warning the government not to allow in chlorinated chicken and hormone-fed beef.
amara Cohen
Political correspondent @tamcohen
SKY NEWS
Monday 15 June 2020 07:22, UK
The government says it is ‘firmly committed to upholding our high environmental, food safety and animal welfare standards outside the EU’
A US trade deal could pose the greatest risk to food safety since the mad cow disease crisis 20 years ago, the government has been warned.
Consumer group Which? has written to International Trade Secretary Liz Truss as a new round of negotiations gets under way between US and UK officials.
The letter, seen by Sky News, raises concerns that the government has changed its stance on animal welfare and food safety in order to strike a US trade deal.
Research by Which? shows that 72% of the British public do not want products such as chlorine-washed chicken and hormone-fed beef to be allowed on sale in the UK at all.
In his election manifesto, Boris Johnson promised the UK would “not compromise on our high environmental protection, animal welfare and food standards”.
Liz Truss is about to enter a second round of trade talks with the US
But recent attempts by MPs to insert a permanent ban into legislation have failed, and ministers are understood to be considering proposals to allow in some of these products
Sue Davies, head of consumer protection and food policy at Which?, told Sky News: “We’re very concerned that the government seems to be backtracking on its commitments.”
Black Lives Matter: Boris Johnson vows to tackle racism – but says we cannot ‘Photoshop the cultural landscape’
Brexit: UK ‘formally confirms’ to EU that it won’t extend transition period
In a letter to Ms Truss, she wrote: “The UK should be proud of the strides we have made over the past two decades to ensure that wherever people buy and eat food it is underpinned by robust safety, quality and welfare standards.
“Since the BSE crisis, the UK has led a food safety revolution that has given us an enviable system across the food chain.
“This could all be at risk depending on the approach that the government takes when it begins a second round of trade talks with the US on Monday.”
Which? urges the government to “leave the issue out of trade deals altogether”, but US trade deals tend to prioritise giving American farmers access to new markets.
In a newspaper article in January, US ambassador Woody Johnson argued that chlorinated chicken is safe and must “absolutely be included” in the talks on a US trade deal.
Consumer group Which? has raised concerns
Free market Tory MPs, including some in the cabinet, are open to overturning the UK’s ban on these products and allowing shoppers to make their own choice.
To prevent UK farmers being undercut, one proposal under consideration is a “dual tariff” system whereby any imported US meat produced using these controversial methods would be slapped with a high tariff.
Meanwhile, produce which meets current UK standards would be charged at a lower rate, or exempt.
Ms Davies said letting these products into the UK at all would create a “two-tier system” whereby cheap food – available in schools and NHS canteens for example – would have lower standards.
Chlorine-washing chicken is done to eliminate infection, and hormones are given to animals to boost yield, but campaigners say these practices allow lower welfare standards and poorer hygiene in the farming process.
‘No health problems with chlorinated chicken’ – govt’s chief scientific adviser
A government spokesperson said: “We remain firmly committed to upholding our high environmental, food safety and animal welfare standards outside the EU, and the EU Withdrawal Act will transfer all existing EU food safety provisions, including existing import requirements, on to the UK statute book.
“These import standards include a ban on using artificial growth hormones in domestic and imported products and set out that no products, other than potable water, are approved to decontaminate poultry carcasses.
“Any changes to existing food safety legislation would require new legislation to be brought before this parliament.”
The spokesperson added that UK food standards are overseen by the Food Standards Agency whose decisions “will be made separately from any trade agreement”.
Ms Truss, who represents a rural constituency in Norfolk, said last month that a US trade deal would represent a “huge opportunity for all farmers” to reach new markets, and that standards would be set so that “British farmers are always able to compete”.
But some senior Tory MPs fear the government is prepared to use its 80-seat majority to end the ban in order to strike a deal with the US.
Today’s second round of talks will last two weeks, with around 100 negotiators on each side meeting remotely.
Environment, Food and Rural Affairs Secretary Theresa Villiers arrives for a cabinet meeting at 10 Downing Street, London.
Theresa Villiers wants the UK to keep its ban on chlorine-washed chicken and hormone-fed beef
Former environment secretary Theresa Villiers wants the UK to keep its ban on chlorine-washed chicken and hormone-fed beef.
She said: “I was very clear that the bans must remain in place. But there seems to have been a change and the government is not giving the assurances which I was that these bans will remain on the statute book.
“An unprecedented coalition of farmers, environmentalists and welfare campaigners are saying we should uphold our values and reflect them in our trade policy.
“Our negotiating team should not sell those short and should be prepared to walk away if the Americans make unreasonable demands.”
The BSE, or mad cow disease, crisis in the 1980s and 1990s was devastating for UK farmers.
Over four million cows were slaughtered to contain the outbreak.
British beef exports were banned by many countries for years afterwards, and it led to much tighter food standards in the UK.
WEDNESDAY JUNE 10TH 2020
Legal action to stop housing development being built on land that was used process cattle during the BSE epidemic near Canterbury, Kent, UK.
‘ BSE rogue prions that cause BSE in animals and the human form of mad cow disease cannot be destroyed by sterilisation, temperature, or time. Rogue prions have no DNA and are virtually indestructible. Living in soil for decades perhaps forever. Plants and other wildlife have been affected. Now houses with gardens in which children will play, flowers and food may grow are being considered by Ashford Borough Council, perhaps councillors and their families would like to live on this land, or the developers children and nearest?’ Christine LORD 10th June 2020
Homes plan at Thruxted Mill near Canterbury faces High Court challenge
KENT TRAVEL NEWS ONLINE
ByGerry Warren
arren@thekmgroup.co.u
Published: 06:00, 01 June 2020
A legal challenge in the High Court has halted a planned housing development on the site of a former animal rendering plant.
It follows the granting of planning permission in 2018 for up to 20 homes at Thruxted Mill at Godmersham, near Canterbury, where cattle infected with BSE – known as mad cow disease – were processed.
Thruxted Mill near Canterbury
There are widespread concerns the ground remains contaminated but the Secretary of State later determined an environmental impact assessment was not necessary.
Now, a High Court judge has ruled that although the minister had recognised the issue of contamination required further investigation, there was a lack of any expert evidence on relevant remediation measures and he “was not in a position to make an informed judgment”
Ashford Borough Council has been told that before the matter can be reconsidered for planning permission, a full environmental impact assessment is required.
The government decision was challenged by local resident Camilla Swire, who said the planning permission was “flawed” and sought legal advice on the environmental aspect of the decision.
“Hopefully this clear-cut case will make a difference to planning and environmental law,” she said.
“Something does need to be done with Thruxted Mill, but the housing as proposed doesn’t make sense.”
Planning and environment specialist solicitor Richard Buxton, who advised Mrs Swire on the challenge, added: “This judgment is a useful ‘red line’. Too often development schemes get away with promises of assessment further down the line and in practice it is very difficult for councils to police them.
“Proper assessment before planning permission tends to lead to better development, respectful of neighbours and the natural environment”.
The plant closed more than 10 years ago, having been a blight on the local community, which complained about the smell and lorries bringing dead livestock to the site.
WEDNESDAY 27th May 2020
A cow in Ireland that died before the farmer called the authorities was diagnosed with Mad Cow Disease on 22nd May 2020. 73 other cows in the herd continue to produce food for human consumption?
BSE is a zoonotic disease like Covid-19 both diseases avoidable caused by global government policies centred on profit not health. Will the current pandemic be a ‘wake-up call’ for global organisations and governments or just two of many lethal man-made diseases we will face over the coming decades? As Trump, Boris Johnson and many other world leaders look towards profit and booming business instead of caring about human, animal health and the importance of our environment.
https://www.oie.int/wahis_2/public/wahid.php/Reviewreport/Review?page_refer=MapFullEventReport&reportid=34431&newlang=en
– IRL 22/05/2020 Alert/Alerte/Alerta – Bovine spongiform encephalopathy/Encéphalopathie spongiforme bovine/Encefalopatía espongiforme bovina

WEDNESDAY 13TH MAY 2020
My article in ‘THERAPY TODAY’ Pandemic Issue was published this month, see link below. Citing the common themes between Covid-19 and BSE, and also the medical students I am working with at University as their mentor/counsellor.
https://www.bacp.co.uk/bacp-journals/therapy-today/2020/may-2020/in-focus/
TUESDAY 14th April 2020
Coronavirus lock down continues in the UK as the deadly zoonotic disease spreads across the globe. Lessons have not been learnt from BSE epidemic, as Toby Ord wrote in the Guardian Newspaper 8th March 2020, ‘our farming practices have created vast number of animals living in unhealthy conditions within close proximity of humans. Many major diseases originate in animals before crossing over to humans’.
Covid-19 is another zoonotic disease just like BSE and the human form of mad cow disease is another disease waiting to explode in the future. Below is an article from Reuters showing how low paid workers in the meat industry are turning up sick because they cant afford not to work and not being given specialised equipment to prevent transmission of the coronavirus as they prepare food for human consumption.
REUTERS 14th April 2020
Low paid workers are the ‘canaries in the mine shaft’ no lessons have been learnt since BSE another avoidable zoonotic disease like Covuid-19. Whilst the rich and powerful remain in their mansions till the virus has ended its deadly course.
‘Elbow to elbow:’ North America meat plant workers fall ill, walk off jobs
Tom Polansek, Rod Nickel
CHICAGO/WINNIPEG, Manitoba (Reuters) – At a Wayne Farms chicken processing plant in Alabama, workers recently had to pay the company 10 cents a day to buy masks to protect themselves from the new coronavirus, according to a meat inspecto
In Colorado, nearly a third of the workers at a JBS USA beef plant stayed home amid safety concerns for the last two weeks as a 30-year employee of the facility died following complications from the virus.
And since an Olymel pork plant in Quebec shut on March 29, the number of workers who tested positive for the coronavirus quintupled to more than 50, according to their union. The facility and at least 10 others in North America have temporarily closed or reduced production in about the last two weeks because of the pandemic, disrupting food supply chains that have struggled to keep pace with surging demand at grocery stores.
According to more than a dozen interviews with U.S and Canadian plant workers, union leaders and industry analysts, a lack of protective equipment and the nature of “elbow to elbow” work required to debone chickens, chop beef and slice hams are highlighting risks for employees and limiting output as some forego the low-paying work. Companies that added protections, such as enhanced cleaning or spacing out workers, say the moves are further slowing meat production.
Smithfield Foods, the world’s biggest pork processor, on Sunday said it is indefinitely shutting a pork plant that accounts for about 4% to 5% of U.S. production. It warned that plant shutdowns are pushing the United States “perilously close to the edge” in meat supplies for grocers.
Lockdowns that aim to stop the spread of the coronavirus have prevented farmers across the globe from delivering food products to consumers. Millions of laborers also cannot get to the fields for harvesting and planting, and there are too few truckers to keep goods moving.
The United States and Canada are among the world’s biggest shippers of beef and pork. Food production has continued as governments try to ensure adequate supplies, even as they close broad swathes of the economy.
The closures and increased absenteeism among workers have contributed to drops in the price of livestock, as farmers find fewer places for slaughter. Since March 25, nearby lean hog futures have plunged 35%, and live cattle prices shed 15%, straining the U.S. farm economy.
North American meat demand has dropped some 30% in the past month as declining sales of restaurant meats like steaks and chicken wings outweighed a spike in retail demand for ground beef, said Christine McCracken, Rabobank’s animal protein analyst.
Frozen meats in U.S. cold storage facilities remain plentiful, but supply could be whittled down as exports to protein-hungry China increase after a trade agreement removed obstacles for American meat purchases.
“There’s a huge risk of additional plant closures,” McCracken said.
The latest came on Monday when JBS [JBS.UL] said it will shutter its Greeley, Colorado, beef plant, which accounts for about 5% of the country’s production, until April 24.
JBS previously had to reduce production at the facility as about 800 to 1,000 workers a day stayed home since the end of March, said Kim Cordova, president of the local United Food and Commercial Workers (UFCW) union that represents employees. She added that the union knew of at least 50 cases and two deaths among employees as of Friday.
Plant worker Saul Sanchez, known affectionately as “grandpa” among some co-workers, tested positive for the virus and died on April 7 at 78 years old, according to his daughter, Beatriz Rangel. She said he only went from home to work before developing symptoms, including a low fever.
“I’m heartbroken because my dad was so loyal,” Rangel said.
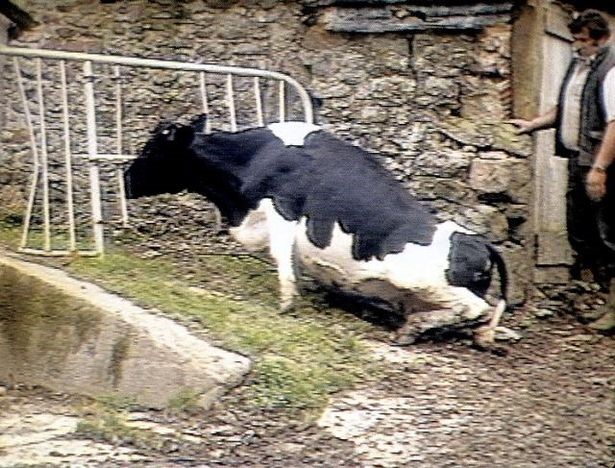
Photo of farm worker with UK cow dying of BSE during the epidemic, many farmers and agriculture workders died of the human form of mad cow disease because they were not protected from the deadly disease.
Tuesday 17th March 2020
The wording the experts and Boris Johnson used during the Coronavirus press conference last evening even the body language of the governments Chief Medical Advisors, had so many similarities and terrible ironies with the handling of the BSE crisis. Lack of leadership, the public unsure, mixed messages, secret meetings and medical science presented as reliable fact.
When over 200 UK top scientists have disagreed with the free movement of UK population during this lethal pandemic.
Last night Johnson and his team, ‘suggested’ that people stay away from public places, cafes, bars, theatre, whilst not putting in strong restrictions to shut these hot-bed of potential infection down. This means all these businesses forced to shut, due to lack of patronage will have great difficulity getting any money from their insurance companies.
Old people over 70 or those with underlying health issues are being told to self-isolate from Friday for up to 3 months. The previous press conference just a few days ago, Johnson and his medical experts stated ‘ we should all continue to go to work and mix until the end of April so that 60 percent of the population acquires Covid-19 and this will bring about ‘herd immunity’.
Unproven theory that would put millions in the UK at risk of dying from the cCvid-19 as there has been no scientific research/ evidence/ fact that a person once recovered from this virus would remain ‘immune’. The number infected and seriously ill some say as many as 4million people if this strategy remains would overhwhelm the NHS.
Schools remain open!
Meanwhile people are allowed and even encouraged to mix freely, when many scientists believe that lock down should have taken place weeks ago. This has strong resonance with how the Tory Government handled the BSE crisis, ‘ wait see, gamnble with the public life and health’, resulting in my son’s needless death. Now in 2020 1 in 2,000 of the UK population carry or incubate the deadly zoonotic disease human BSE. BSE remains in our animals, waiting to explode in humans, and decimating deer, moose and other animals with it sibling disease CWD across USA, Canada and Europe.
Lock down in UK regarding Covid-19 is the only way to prevent deaths. The public have started hunkering down voluntarily as work organisations protect their staff, by ensuring they work remotely from home. Yet no guidance from the UK government.
Coronavirus sweeps across England, Scotland, Wales, Northern Ireland, Eire. Numbers of infections continue to rise and people continue to die of Covid-19.
UK government remains weak, uncertain and allowing the public to make decisions without the backing of an economic plan to prevent millions of people losing their jobs.
Apparently the government is buying private beds from private health care hospitals for the NHS at over £24 m a day. Another scandal, with many in the establishment having shares in private health care and insurance.
I will write another blog when I feel it’s the right time. A huge wave a deadly virus called
Covid-19 will cross and destroy many people’s lives very soon, another zoonotic disease which could have been prevented just like BSE. How many more needless deaths this time?
Once again ordinary people will suffer and die, due to greed, UK and global government policies caring more about shareholders, big business making money than the environment, human and animal health.
I hope with all my heart that once this is over a ‘new world order’ of decent politicians and policy makers with the support of activists and campaigners will make sure this never happens again and that our beautiful planet and lovely global family with all its people, animals, plants and life can finally breathe fresh air not pollutted by the many that hold power that care only about making money and value nothing that really matters.
Andrews baby shoes
Monday 16th March 2020 (morning)
The global pandemic caused by a new deadly coronavirus, named Covid-19 is sweeping the world, killing people and infecting hundreds of thousands. The strategies being used by the current UK government and its Prime Minister Boris Johnson, echoes the ‘wait and see’ policy that blanketed the BSE epidemic. Currently the British Government is allowing the UK public to go about their daily lives spreading the infection. Schools remain open, people are being actively encouraged to attend events with thousands of participants. Therefore enhancing and enlarging the deadly virus withing UK communities. Those that are infected but not showing symptoms are creating a ‘whirlwind’ of needless seriously ill patients which the NHS will not be able to cope with. People will die alone at home with no medical intervention whilst Boris Johnson the rich and powerful will have the best health care and will ‘lock down’ during the worst of this pandemic.
As of this morning UK has over 1,100 positive cases of coronavirus and 35 people have died. The UK current Medical Officer is telling the UK public that allowing the infection to spread within our communities will result in a ‘herd immunity’ meaning 60 percent plus of people in the UK will become infected. There is no proof that Coronavirus provides ‘immunity’ once a person has recovered from the infection.
Over 200 hundred experts in infectious diseases, have stated that ‘herd immunity theory’ regarding coronavirus has not been tested and will result in millions of people becoming seriously ill and possibly 500,000 UK people’s needless deaths.
Professor Roy Anderson told Thatcher during BSE that the way to contain the deadly mad cow disease was to test, trace and isolate. The proven way to beat any epidemic. He was interviewed by BBC1 last Friday and stated ‘ his alarm at the UK policy regarding Covid-19’. Boris Johnson and his Conservative Government Policy is enhancing the infection and deaths.
Test, trace and isolate, has worked in China and in South Korea and has worked numerous times with other deadly infections. In China where the Coronavirus began the death rate has dramatically fallen, in South Korea this is happening too. The way to handle any deadly infection in humans is to test, trace and isolate not to amplify by allowing communities to mix with large groups.
Once again economics is coming before human health and the UK Prime Minister Boris Johnson and his advisors are more concerned about infecting as many people in the UK as possible, people dying quickly so that those left can return to work asap. This is another experiment by a Conservative Government in the same way that BSE was allowed free reign during the 1980s and 1990s.
https://www.theguardian.com/commentisfree/2020/mar/15/uk-covid-19-strategy-questions-unanswered-coronavirus-outbreak?CMP=share_btn_link
WEDNESDAY 5th FEBRUARY 2020
Cow aged 13 years found with BSE in SwitzSwitzerland reports atypical BSE case in farm cow – OIE …
www.reuters.com/article/us-health-bse-switzerland-idUSKBN1ZZ2KN
PARIS (Reuters) – Switzerland has reported a case of atypical bovine spongiform encephalopathy (BSE) in a farm cow, the World Organization for Animal Health (O
Information received on 05/02/2020 from Mr Hans Wyss, Chief Veterinary Officer, Schwarzenburgstrasse 161, Swiss Federal Veterinary Office, LIEBEFELD BERNE, Switzerland
Summary
Report type Immediate notification (Final report)
Date of start of the event 29/01/2020
Date of confirmation of the event 03/02/2020
Report date 05/02/2020
Date submitted to OIE 05/02/2020
Date event resolved 03/02/2020
Reason for notification Recurrence of a listed disease
Date of previous occurrence 03/2012
Manifestation of disease Clinical disease
Causal agent Prion (atypical BSE type L)
Nature of diagnosis Laboratory (advanced)
This event pertains to the whole country
New outbreaks (1)
Outbreak 1 Einsiedeln, Schwyz
Date of start of the outbreak 29/01/2020
Outbreak status Resolved (03/02/2020)
Epidemiological unit Farm
Affected animals
Species Susceptible Cases Deaths Killed and disposed of Slaughtered
Cattle 68 1 0 0 1
Summary of outbreaks Total outbreaks: 1
Total animals affected
Species Susceptible Cases Deaths Killed and disposed of Slaughtered
Cattle 68 1 0 0 1
outbreak statistics
Species Apparent morbidity rate Apparent mortality rate Apparent case fatality rate Proportion susceptible animals lost*
Cattle 1.47% 0.00% 0.00% 1.47%
*Removed from the susceptible population through death, destruction and/or slaughter
Epidemiology
Source of the outbreak(s) or origin of infection
Unknown or inconclusive
Epidemiological comments
Confirmation of atypical Bovine spongiform encephalopathy (BSE) in a cow on 3 February 2020. The 13 year old cow from a holding in the Canton of Schwyz was subject to emergency-slaughter on 23 January 2020. Samples of the brain stem were sent in for analysis and confirmed at the Swiss National Reference Laboratory for Transmissible Spongiform Encephalopathies. The sample tested positive in the rapid test for BSE “Priostrip BSE” and was confirmed by Western lmmunoblot. The pathological prion protein could be classified as (L) -Type BSE and therefore as an atypical case of BSE. The entire carcass was disposed of as category 1 material.
Control measures
Measures applied
Vaccination prohibited
No treatment of affected animals
Measures to be applied
No other measures
Diagnostic test results
Laboratory name and type Species Test Test date Result
National Reference Laboratory (National laboratory) Cattle western blot 03/02/2020 Positive
Future Reporting
The event is resolved. No more reports will be submitted.
https://www.oie.int/wahis_2/public/wahid.php/Reviewreport/Review?page_refer=MapFullEventReport&reportid=33179&newlang=en
December 2019
‘The future of the vCJD epidemic is still uncertain, with recent estimations of 1 carrier of prion infection in every 2,000 persons who lived in the United Kingdom during the BSE epidemic (32). However, in a recent update from the same group, prions were detected in a cohort of persons born after the BSE epidemic, suggesting that the number of silent carriers of prions might be higher than originally anticipated.’
Monday December 16th 2019
This is the day my only son Andrew died, he was unlawfully killed by the Human BSE, at 9.25pm in the evening in 2007, he was just 24 years old. Human BSE, vCJD, the human form of mad cow disease, now repackage as prion disease. Even though as a family we had not eaten beef since 1988. But bovine material is in every part of the human food chain/environment, from toothpaste, medicines to baby cough mixture and vaccines.

Photo Andrew aged 18months his first Christmas snow with mum Christine
My son’s once healthy young body and brain was systematically destroyed over many months by the rogue prions that cause Human BSE. He went from a young man working in London in the media, full of life, promise and a great future to becoming totally paralysed with dementia within months of the disease symptoms becoming apparent. His healthy young brain was literally punched with holes by the lethal mis-folding prion that causes Human BSE.

Photo Andrew aged 21 years central London working for TalkSPORT UK national radio station
The consumption of infected beef, bovine material or ingestion via vaccines have been cited as the culprit. There has never been a court case to determine those responsible for the unlawful death of my son and so many other innocent people. There has been ‘ no duty of care’ accepted or recognized by UK government ministers, scientists, officials, food and pharmaceutical corporation who allowed these lethal agents into the human food and medicine chain. Now 1 in 2,000 or more of the UK population many born after the BSE epidemic are either carrying or incubating the human form of mad cow disease, a legacy that has sprouted other prion disease in animals such (CWD) Chronic Wasting Disease in the USA in deer ( known as BSE on steroids). Globally we all face a ticking health-time bomb with the amount of lethal BSE/CWD material being processed into the human/animal food chain in 2019.
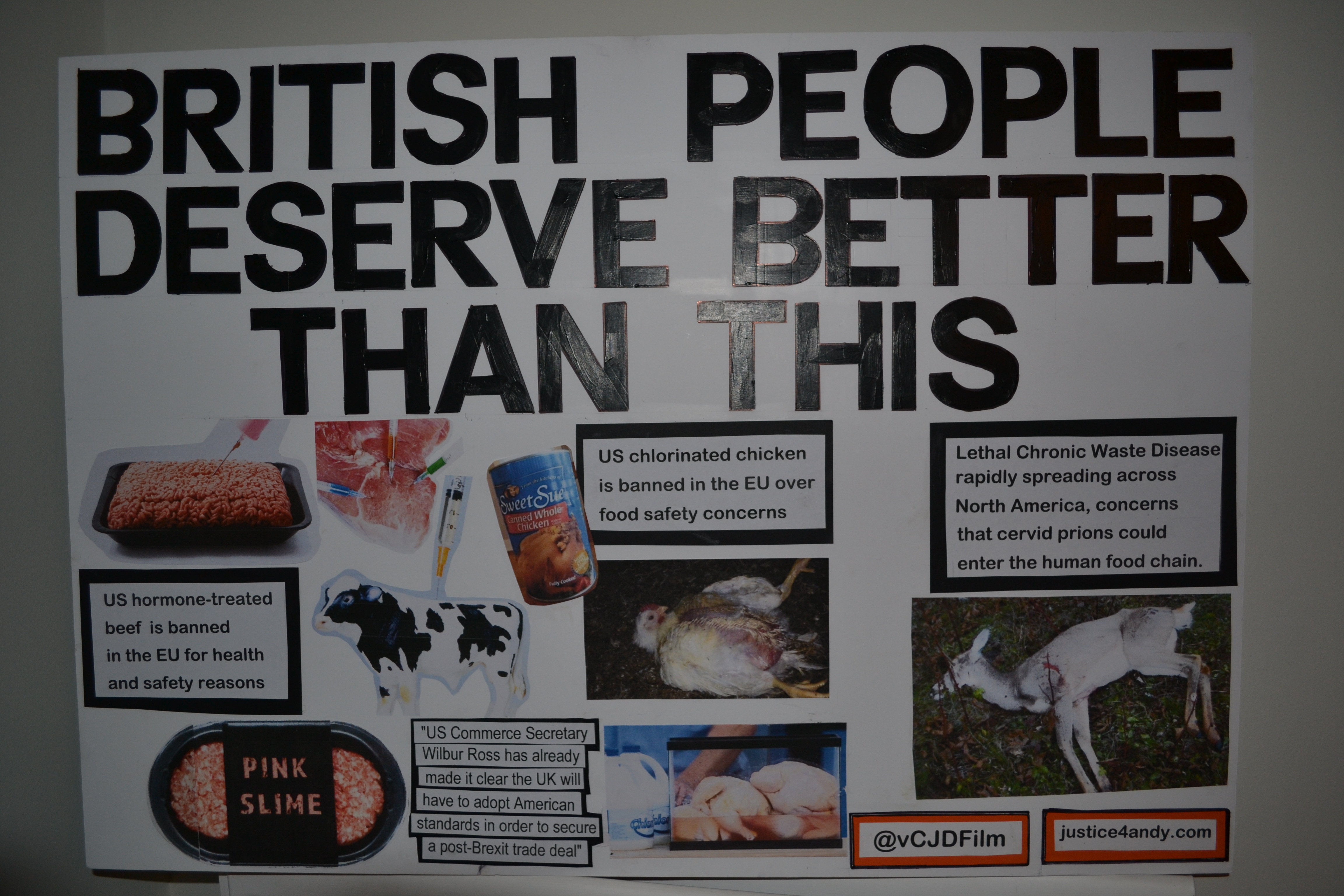
Placard/poster for www.justice4andy.com campaign at the recent demonstrations in central London 2019
All food and medicines for human consumption should never kill, and if they do those responsible should face criminal proceedings. This has never happened, as with the powerful, wealthy and influential those in the frame for the corporate manslaughter of my only son Andrew, have been given a ‘get out of jail free card’ first with the Phillips/BSE inquiry and since by the many cronies and officials also implicated, the creatures of the night that still in (2019) stalk/manage Whitehall and care little about members of the public, only money, promotion and keeping those in the establishment ‘above the law.’ As an investigative journalist I continue to uncover the truth about Human BSE its origins, those responsible and the lethal prion disease BSE and its many strains such as CWD Chronic Wasting Disease in deer, elk, reindeer and moose.

Photo Andrew as a 4 year old having fun on the beach
With the recent general election in the UK (12th December 2019) and the Conservative majority, the same cronies, mindset that allowed BSE to run riot in our food/medicine chain exists today. With the Conservative Party and Prime Minister Boris Johnson seeking a deal with Donald Trump to send knock down untested BSE US beef to the UK and venison from herds affected by CWD! The USA under Donald Trump has sacked hundreds of scientists/experts in human mad cow disease/animal disease, there are also no precautionary principles regarding food safety in the USA. These lax regulations will be coming to UK shores so that once again the food corps and pharmaceutical giants will make a lot of ‘dollar’, at the risk of global human and animal health and well-being.

Andrew far left with friends
Today I remember my son for the handsome, happy, and full of life young man he was but, also the life he should have lived, the people he should have met, over sixty years of living he was denied.

Photo Andrew working in the studios aged 21 years old with best friend Sean Dilley (BBC)
Those that are named and shamed on this website who cared so little for my son and other victims lost lives and dreadful, painful deaths, are still being investigated by myself and other journalists. Despite the threats. Intimidation and bullying by those responsible, I continue with my quest for justice and the truth.
My son was killed by corporate greed, ministerial knowledge that was hidden to protect the money making machines that are the food and drug industries.
One day in the not too distant future these men and women and their implicated family friends, cronies and employees will be brought to account in a court of law.
Crying is a way your eyes speak
When your mouth can’t explain how
Broken your heart is. (Anon)

Photo happy times with sister Emma, Andrew and mum Christine
Remembering my Andrew with love, affection and longing always for him to be here alive, well and living his life with me his Mother, Sister Emma, friends, work colleagues and family.
‘On winter evenings when the mist hangs low
Over the reed beds and the reeds look blue
And chill, chill, chill
The wild ducks call each other
I shall remember you.
(Anon 5th Century Japanese)
Photo Andrew aged 23 2006
Always holding your hand, my beloved boy Andrew. Mum x
TUESDAY DECEMBER 10th 2019
Preclinical Detection of Prions in Blood of Nonhuman Primates Infected with Variant Creutzfeldt-Jakob Disease
Volume 26, Number 1—January 2020
Research
Preclinical Detection of Prions in Blood of Nonhuman Primates Infected with Variant Creutzfeldt-Jakob Disease

MONDAY DECEMBER 9th 2019
https://www.thesun.co.uk/news/10471697/sickness-mad-cow-disease-spreading-deer/
I have been involved in the filming, research and contributed to a new Canadian film called ‘No Accident’ see details below. Chronic Wasting Disease in the USA is a pandemic among deer herds. CWD is the equivalent of BSE on steriods and poses lethal dangers to animals and humans. Deer hunters have been reported as developing symptoms similar to vcjd and meat from affected CWD deer herds have ended up in the human food chain, namely food banks to support the poor. Huge fires and pyres of dead deer suffering from CWD have been torched across many states in the USA, the similarties to BSE is astounding, shocking and deeply concerning for human, animal health. Please take the time to watch the trailer of ‘No Accident’ the full film will be broadcast in 2020.
No Accident is one such story.Over explicit warnings by scientists that domestication fosters and accelerates diseases, game farming was legalized in much of North America in the late 1980s. Epidemics emerged almost immediately. The latest is Chronic Wasting Disease (CWD), an elk and deer version of ‘mad cow.’ Untestable, untreatable …
THURSDAY OCTOBER 31st 2019
BREXIT has now been extended to January 31st 2020 and with a general Election taking place in the UK on 12th December 2019, the UK is unsettled and chaotic and divisive in its politics, class and social awareness.
Trump has been having ‘secret’ talks with various UK ministers over cheap meat heading to the UK from USA shores. As the USA has no precautionary principle over its health and safety standards for its meat, knock down USA meat harbouring lethal and dangerous toxins and disease will be heading to our supermarkets post BREXIT, Only 20,000 US cattle are tested annually in the USA for BSE and there are 95 million head of cattle in America. Trump has and continues to cut experts, scientists in animal disease, and since the beginning of his tenure has shut down many scientific facilities which used to test and keep check of domestic and animal disease across the USA.
Below is news that the USDA is no longer considering tagging animals in the USA, ‘feeder cattle’ are also omitted from this proceedure. This will allow free movement of diseased, ill, potentially BSE infected aninmals.
T Kate Richer died of human mad cow disease
Kate Richer died of human mad cow disease
Cow dying of mad cow disease, would you eat this meat or give it to your kids for tea?
Trumps secret talks also include the privatisation of the NHS, there are huge amounts of money at stake for rich buisness people and US organisations to make a ‘killing’ at the expense of the UK public, especially the young, vulnerable, poor and the old. The Daily Mirror headline news today is ‘BORIS AND TRUMP PLOT NHS SELL-OFF’ with the drive of US big Pharma companies hiking the price of medicines. Health and health care will then become only available to the rich and those with private health care. It will be the death-knell for the NHS and for many working class and poorer UK citizens and their families.
Boris Johnson and Donald Trump plot to sell-off NHS in £27bn trade carve-up
The Labour Party leader fears the health service could be thrown open to Big Pharma companies after Brexit
The NHS is at critical risk as Boris Johnson wields the national treasure as bait in trade talks with the US, Labour claims.
The health service could be forced to pay a crippling £500million a week more for medicines if thrown open to Big Pharma companies post-Brexit.
Labour leader Jeremy Corbyn today accuses the Tories of putting the NHS “up for grabs” as he launches Labour’s election campaign.
He pledges never to allow Donald Trump to get his hands on the health service for US firms in a trade deal.
It follows revelations that senior British civil servants have been in secret talks with US firms to discuss the NHS in preparation for a post-Brexit trade deal.


On the day the Prime Minister had promised a “do or die” Brexit , the Labour leader will say: “ Boris Johnson ’s planned sell-out deal with Donald Trump means yet more NHS money taken away from patients and handed to shareholders.
“The NHS is up for grabs by US corporations in a Trump trade plot.
“It has been revealed that the cost of drugs and medicines has repeatedly been discussed between US and UK trade officials. Labour won’t let Donald Trump get his hands on our National Health Service.”
As long ago as January, America’s pharmaceutical firms were asking the US government to ensure Brexit trade negotiations increased the price they can charge the NHS for drugs.

At a public hearing in Washington DC, Brian Toohey of the Pharmaceutical Research and Manufacturers of America moaned about price controls set by Britain. He went on to say the US-UK Brexit trade negotiations were “an important opportunity” to force the UK to pay the higher drug prices US manufacturers are desperate to charge.
He demanded “full market access for US products” and “competitive market-derived pricing”.
Without the price controls the NHS could be forced to pay hugely inflated American costs – which can be over 20 times more for some medication, costing the NHS billions.
Dr Andrew Hill of the University of Liverpool, an advisor to the World Health Organisation, said: “Our annual drugs bill for the NHS is £18 billion. If we had to have American drug prices we are talking about that going up to £45billion – or £500million a week extra for the NHS to pay.” When the PM went to the US in September he planned to tell business leaders Britain will roll out the red carpet for a trade deal, with tax breaks and fast-track public sector contracts.
And in June, Trump told a press conference in the Foreign Office: “I think everything with a trade deal is on the table. So NHS or anything else…everything will be on the table, absolutely.”
Mr Johnson, Health Secretary Matt Hancock and International Trade Secretary Liz Truss have all insisted the NHS is “off the table” in talks with the US when UK leaves the European Union.
TUESDAY, OCTOBER 29, 2019
USDA Abruptly Halts Animal ID Plan As Experts Testify USA Underprepared For Bioterrorism Threats Such As BSE TSE Prion aka Mad Cow Disease
MONDAY OCTOBER 7th 2019
https://www.independent.co.uk/news/uk/politics/boris-johnson-brexit-environment-rules-trump-trade-deal-a9143221.html
“the international trade secretary, said scrapping the protections was “vital for giving us the freedom and flexibility to strike new trade deals and become more competitive”.
With the lowering of environmental and food safety standards to secure a deal with Trump/ USA after BREXIT, this will mean even more lethal diseases will be coming to a supermarket near you!
The USA have no precautionary principle regarding their food industry so it means animals that are called ‘downers’ that collapse due to exhaustion, illness or disease regularly enter the US human food chain. 95 million cattle in the USA and only 20,000 a year are tested for BSE and US cattle are still getting mad cow disease.
Across most of the states in Amercia deer, moose, elk and other wild animals that are being domesticated for human consumption are dying and developing CWD chronic wasting disease which is what experts call ‘BSE in steroids’. Deer with obvious symptoms are killed whilst the rest of the herd is being used to feed families across the US. Deer hunters are experiencing similar symptoms of cjd/human BSE. Yet the US government continues to look away.
A lethal pandemic in deer and other animals is scorching across the US and with a trade deal with TRUMP it be heading to UK shores post BREXIT. Photo below is of young UK mum Sally who was dying of the human form of mad cow disease when she gave birth to her baby daughter Emily. Emily from birth has been disabled, Emily cannot speak, walk or eat. This is the reality of lower food standards to make the rich and shareholders richer whilst putting you and your family at risk.

SUNDAY 22nd SEPTEMBER 2019
Today I took part in the Brighton and Hove demonstration regarding food safety, women4europe and anti Brexit. There were hundreds of people marching along the seafront as the annual Labour Party Conference was taking place. Here are some photos above, me with union leader Len MCCluskey and below various other individuals and groups who took part. Never has the UK been more divided but, the demonstration brought lots of communities together all wanting a better future for our children and granchildren, A place where the air is clean, climate is considered, animal health is paramount and human health and our lives and families lives number one consideration and the profit of the few does not impact on the many.

Monday 2nd September 2019
Today is my son Andrew’s birthday, he was born at 1.20pm on 2nd September 1983.
Time does not heal the pain. The yearning to hear, see, touch and cuddle my beloved boy Andrew grows with each passing day, week, month and year. I cannot imagine my son a mature man as he died of human BSE when he was just 24 years old. On the brink of so much life and potential.

Andrew was my number one son, his sister Emma misses him more than ever.
Love always Andrew from Mum and Emma xx
“It’s so much darker when a light goes out than it would have been if it had never shone.”
–John Steinbeck, The Winter of Our Discontent
THURSDAY 8th AUGUST 2019
ROYAL ACADEMY OF ARTS SUMMER SHOW LONDON JUNE-12th AUGUST 2019
Christines documentary Cows, cash and cover-ups? featured as part of Roger Hiorns art
www.vanityfair.com/london/2019/06/the-a-list-the-best-culture-to-catch-this-week
PORTSMOUTH NEWS
A GROUND-BREAKING documentary about the human form of Mad Cow Disease (BSE) – co-produced by a Portsmouth journalist – will be included in London’s Royal Academy of Arts’ Summer Exhibition this year.Cows, Cash & Cover-ups? Investigating vCJD (Creutzfeldt-Jakob Disease), explores calls for a criminal inquiry to be held to examine the handling of the BSE crisis by the government and authorities in the farming and food industries. The film also asks how Brexit could escalate food safety problems.
Award-winning Portsmouth investigative journalist Christine Lord acted as associate producer. Lord lost her only son Andrew Black to the human variant of the disease vCJD in 2007 when he was just 24 years old.
 Ian Reddington narrator of Christine’s documentary Cows, cash and cover-ups?
Ian Reddington narrator of Christine’s documentary Cows, cash and cover-ups?
Lord published a book Who Killed My Son? and launched justiceforandy.com to expose how the disease took so many lives.
Ian Reddington, known for Outlander, EastEnders and Coronation Street, narrated the independent documentary.
 Christine with Roger Hiorns
Christine with Roger Hiorns
The film will form part of artist Roger Hiorns’ work ‘A Retrospective View of the Pathway’ at the Royal Academy.
UK Film Review has awarded the documentary five stars out of five. The review said: ‘A vital, urgent and frightening raising of an issue that we should all make it our duty to know about.
‘This documentary should be televised on the grandest scale and its story shared with as wide an audience as possible.
‘Scary and upsetting, Cows, Cash & Cover-ups? Investigating vCJD is essential coverage of an important but under-discussed subject people would rather believe a tragedy of the past, than a fear of the future.. The film is the first step into changing this mindset and is one hell of a powerful and well-researched achievement.’
Around one in every 2,000 people in the UK may carry vCJD proteins, according to a study published by the British Medical Journal. Long incubation periods for the disease mean that the true number of possible victims is unknown.
The Summer Exhibition is the world’s largest open submission art show and has been running without interruption since 1769.
The show runs from June 10 to August 12, 2019.
FRIDAY AUGUST 2nd 2019
Trump, EU officials announce deal to sell more American beef to Europe
WASHINGTON (Reuters) – U.S. President Donald Trump announced a deal on Friday to sell more American beef to Europe, a modest win for an administration that remains mired in a trade war with China, but he said tariffs on European auto exports remain a possibility.
The European Commission has stressed that any beef deal will not increase overall beef imports and that all the beef coming in would be hormone-free, in line with EU food safety rules. The deal needs European Parliament approval.
“The agreement that we sign today will lower trade barriers in Europe and expand access for American farmers and ranchers,” Trump said at a gathering of European Union officials and cowboy-hatted American ranchers in the White House Roosevelt Room for the announcement.
The agreement was then signed by U.S. Trade Representative Robert Lighthizer, Stavros Lambrinidis, the European Union’s ambassador to the United States and EU representative Jani Raappana.
Trump joked that his administration was working with the EU “on a 25% tariff on all Mercedes-Benz and BMWs coming into our nation.”
“So, we appreciate – I’m only kidding,” he said to laughter.
But talking to reporters later, he said imposing the tariffs on European autos remained a possibility.
“Auto tariffs are never off the table,” Trump said. “If I don’t get what I want, I’ll have no choice but maybe to do that. But so far they’ve been very good.”
The beef deal could help alleviate some of the damage to the domestic agricultural industry because of tariffs Beijing has imposed on U.S products in retaliation for U.S. levies on China.
 BBC News October 2018 report of cow with BSE Scotland UK.
BBC News October 2018 report of cow with BSE Scotland UK.
Trump said in the first year duty-free U.S. beef exports to the EU will increase by 46% and over seven years will rise 90% further. “In total the duty-free exports will rise from $150 million to $420 million, an increase of over 180%,” he said.
Without mentioning China by name, Lambrinidis said the United States and Europe could work together to stand against countries that did not compete fairly in the global market.
“The agreement shows us that as partners we can solve problems,” he said.
QUOTA
EU sources and diplomats in June said a deal had been reached to allow the United States a guaranteed share of a 45,000 tonne European Union quota.
There are 17 U.S. slaughterhouses approved to export beef to Europe, run by companies including Tyson Foods Inc, National Beef Packing Company [NBEEF.UL], Greater Omaha Packing and JBS USA’s [JBS.UL] Swift Beef Company, according to U.S. Department of Agriculture records.
“Our ability to participate in trade with the EU over the years has been challenged by limitations,” Tyson said. “This agreement provides the opportunity for a more consistent flow of high quality beef product to meet customer and consumer demands.” Opportunities for U.S. meat producers to export beef to the EU under the quota have been inconsistent as other suppliers such as Australia, Uruguay and Argentina have been approved to ship under the quota. The U.S. beef industry believes spotty access to the market is a reason why more American farmers do not raise their cattle without hormones, which speed up growth. The EU bans beef from cattle treated with synthetic growth hormones.
The biggest problem with the European market has been the uncertainty,” said Kent Bacus, director of international trade for the National Cattlemen’s Beef Association, an industry group. U.S. farmers have suffered from trade disputes with other trading partners, including China and Mexico. China last year imposed retaliatory tariffs on American farm goods including pork.
Friday’s announcement coincides with Trump ratcheting up Washington’s trade dispute with China. On Thursday, he said he would impose a 10% tariff on $300 billion of Chinese imports from Sept. 1 and threatened to raise tariffs further if Chinese President Xi Jinping failed to move faster on striking a trade deal.
The dispute between the world’s two top economies has hurt world growth, including in Europe, as it enters its second year.
U.S. and European officials have sought to lay the groundwork for talks on their own trade agreement but have been stymied over an impasse on agriculture.
The agreement on beef could, however, ease tensions between the two sides, which are each other’s largest trading partners.
Uk cow dying of mad cow disease (USA has over 95 million cattle just 20,000 annually are tested for BSE and they still find cases!) (2019) (Christine Lord research 2019)The Trump administration has been pursuing a host of new trade deals with Europe, China and others as part of the Republican president’s “America First” agenda as he seeks a second term in office, but difficulties in securing final pacts have roiled financial markets.
European stocks on Friday were battered by Trump’s latest salvo against China and Wall Street also took a hit.

UK protestors banner, people’s march 2019

TUESDAY 17th JULY 2019
Cow in SPAIN with BSE 5th July 2019
Where is the research that says that atypical BSE is spontaneous and nothing to do with human mad cow disease? Would anyone in their right mind eat any of the other cattle in this infected herd? Well some families are, as many of the cattle in that herd have already gone to market.
Monday 16TH JULY 2019
My new documentary cows, cash and cover-ups? investigating vcjd is now part of this years Royal Academy of Arts Summer show until August 12th 2019 in central London.
PRESS RELEASE
vCJD / Mad Cow Disease Documentary Included in Royal Academy of Arts’
Summer Exhibition 2019
FOR IMMMEDIATE RELEASE
A ground-breaking documentary about Variant Creutzfeldt-Jakob Disease (vCJD), the human
form of Mad Cow Disease (BSE), will be included in London’s Royal Academy of Arts’
Summer Exhibition 2019.
‘Cows, Cash & Cover-ups? Investigating vCJD’ explores calls for a criminal inquiry to be held
to examine the handling of the BSE crisis by the government and authorities in the farming
and food industries. The film also asks how Brexit could escalate food safety problems.
Ian Reddington (known for Outlander, EastEnders and Coronation Street) narrated the
independent documentary.
narrator Ian Reddington
The film will form part of artist Roger Hiorns’ work ‘A Retrospective View of the Pathway’ at
the Royal Academy. He was invited to participate in the exhibition by artists, curators, and
Royal Academicians, Jane and Louise Wilson.
Hiorns presents a simple and stark work that displays a QR code link to the film on an A4
polyester adhesive label.
The Royal Academy is a traditional establishment that has now shown its openness to this
new work, marking an exciting and thoughtful decision and one welcomed by the artist.
Hiorns said, ‘If the timeline of art that stretches into the future still values progress, the
vCJD work would occupy the sculptural space alongside a Richard Long or a Henry Moore. It
would deepen the understanding of our contemporary conditions of being in the world, and
participate in the desire to reorganise structures of hierarchy embedded into art history so
far.’
The film documents the experiences of families of victims who contracted the fatal disease.
Interviews with families from across the UK are featured alongside activists, artists, farmers,
professors and scientists.

Christine with director of Cows, cash and cover-ups? Joseph Mclean
UK Film Review has awarded the documentary five stars out of five, describing it as, ‘A vital,
urgent and frightening raising of an issue that we should all make it our duty to know about.
This documentary should be televised on the grandest scale and its story shared with as
wide an audience as possible.
‘Scary and upsetting, Cows, Cash & Cover-ups? Investigating vCJD is essential coverage of an
important but under-discussed subject people would rather believe a tragedy of the past,
than a fear of the future. [Director] McLean’s film is the first step into changing this mindset
and is one hell of a powerful and well-researched achievement.’
Joseph Andrew McLean of Partickular Films in Glasgow directed the documentary.
2
Sutdent Kate Richer died of vcjd aged 22 years old, Kate’s parents are interviews in the film.
Award-winning Portsmouth investigative journalist Christine Lord acted as associate
producer. Lord lost her only son Andrew Black to vCJD in 2007 when he was just 24 years
old. Lord then published her book ‘Who Killed My Son?’ and launched justiceforandy.com to
expose how the disease took so many lives.
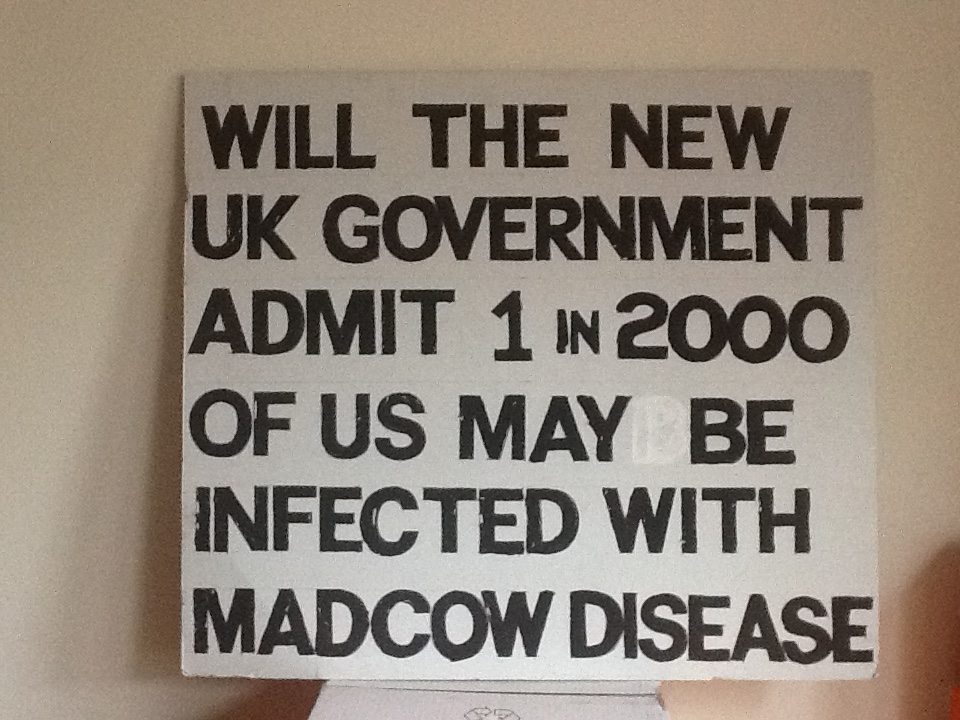
H1 in 2,000 carry vcjd
Around 1 in every 2,000 people in the UK may carry vCJD proteins, according to a study
published by the British Medical Journal. Long incubation periods for the disease mean that
the true number of possible victims is unknown.
Cows, Cash & Cover-ups? Investigating vCJD is available on Amazon Prime and Vimeo. It was
selected for the 2018 Edinburgh International Film Festival’s Distribution Rewired
programme.
The Summer Exhibition is the world’s largest open submission art show and has been
running without interruption since 1769.
It brings together art in all mediums by leading artists, Royal Academicians and household
names as well as new and emerging talent. Around 1,200 works will be on display, most of
them for the first time.
Andrew aged 23
Hiorns’ work looks deeply at the conditions of being and of the conditions of being human.
He examines closely the form of the human under pressure, and of the human in transition,
physically and materially. He also proposes an inceptual approach to art making, in which he
proposes the next form and formality of art making itself.
The show runs from 10 June – 12 August 2019.
FREE ACCESS TO THE FILM FOR REVIEW PURPOSES:
Please contact Joseph Andrew McLean (details below)
PUBLIC (PAID) ACCESS TO THE FILM:
AMAZON PRIME: https://www.amazon.co.uk/Cows-Cash-Cover-ups-Investigating-vCJD/dp/B07R3DR6ZK/
VIMEO: https://vimeo.com/ondemand/cowscashcoverups
MONDAY April 8th 2019
My shocking 1 hour 14min documentary Cows, cash and cover-ups? investigating vcjd has been released. Please log on watch the free trailer and then see the film. (links below) Find out why BSE has not gone away, find out about mad cow disease and its lethal consequences for all of us in 2019 and beyond.
Read the 5***** UK Film review.
Here’s the link to Vimeo on Demand –
https://vimeo.com/ondemand/cowscashcoverups
UK Film Review reviewed Cows, Cash & Cover-ups
https://www.ukfilmreview.co.uk/blog/cows-cash-cover-ups-investigating-vcjd-film-review
‘this film is a hard watch but a necessary one and it asks some serious questions about what goes in our food,
how much we know about this (and for that matter…anything), the international aspects of meat management and the reprehensible ethics of those running the show’
‘This is not so much a film as a sounding of the alarm and it is a vital, urgent and frightening raising of an issue that we should all make it our duty to know about.
This documentary should be televised on the grandest scale and its story shared with as wide an audience as possible’
SOCIAL MEDIA COWS CASH AND COVER-UPS? Investigating vcjd
If you follow/subscribe to the official social media profiles below, you’ll get further updates:
FACEBOOK – https://www.facebook.com/CowsCashAndCoverups/
TWITTER – https://twitter.com/vCJDFilm
INSTAGRAM – https://www.instagram.com/vCJDFilm/
TRAILER
Vimeo link to share – https://vimeo.com/203115042
IMDB: https://www.imdb.com/title/tt4496420/
Monday 25th February 2019
Professor Richard Lacey who warned that Mad Cow disease would infect humans has died aged 77 years old. For many years he suffered, ridicule, threats and bullying by the very ministers that created and condoned BSE entering the human food chain. In 2019 1 in 2,000 of the UK population now carrying or incubating human mad cow disease, Lacey’s scientific predictions prooved to be even more relevant in 21st century. If Laceys warning had been heeded my son Andrew and many other victims of human BSE may not have been infected.
The Telegraph Obits
Professor Richard Lacey, microbiologist rubbished but later vindicated for warning that BSE could be transmitted to humans – obituary
21 FEBRUARY 2019 • 8:32PM
Professor Richard Lacey, who has died aged 78, was the dissident Leeds University medical microbiologist who in 1990 first alerted the British public to the link between the cattle disease Bovine Spongiform Encephalopathy (BSE or “Mad Cow Disease”) and its human equivalent, Creutzfeldt-Jakob Disease (CJD).
Warning of a future of hospital wards full of “thousands of people going slowly and painfully mad before dying”, he called in a Sunday Times interview for the slaughter of all BSE-infected herds (translated by the paper into the headline, “Leading Food Scientist Calls for Slaughter of 6 Million Cows”). The article provoked a carpet bombing of reassuring press releases from the Ministry of Agriculture…
https://www.telegraph.co.uk/obituaries/2019/02/21/professor-richard-lacey-microbiologist-rubbished-later-vindicated
Sunday 3rd February 2019
John Gummer was at the heart of the BSE crisis allowing BSE infected material to feed millions across the UK and globally. He continues with the cover-ups and corruptions surrrounding every aspect of the BSE/mad cow disease and subesequent thousands of unlawful deaths due to BSE infected material being ingested or consumed by innocent members of the public.
His daughter rightly refused to eat the beefburger Gummer tried to make her eat in 1990. Gummer as always protects his career and fincances and will scarifice anything or anybody ( other than himself) as long as he continues his lucartive career and financial gains.
MAIL ON SUNDAY by David Rose 3rd February 2019
Tory peer in £600,000 conflict of interest: Climate Change chief John Gummer faces calls to quit over payments from ‘green businesses’ to his family firm where daughter he famously fed a beef burger during the height of the BSE crisis is a director
- Conservative peer’s family-run consultancy been paid huge sums by businesses
- MPs say Mr Gummer should have declared the payments – but he never has
- He last night denied conflict of interest and said complied with disclosure rules
 John Gummer
John Gummer
Friday 1st February 2019
See my blog/BBC report below US corporations want UK to lower food beef and drug standards post Brexit which means huge profits for USA/UK food/drug companies but a lowering of food and safety health standards.
This is a photo of a cow dying of mad cow disease, the symptoms suffered from these distressed and disabled animals are the same symtoms suffered by humans when they contract Human BSE from eating/ingesting contaminated meat, vaccines, medicines, blood, tissues, donated organs or via medical proceedures such as operations, dentist proceedures. 1 In 2,000 of the UK population now carry incubate human mad cow disease/vcjd and with incubation periods upwards of 50 years, these indivdiuals can be ‘silent carriers’ but able to pass it onwards to others via medical proceedures/blood donation/blood products.
BBC NEWS
US firms seek changes to UK standards on beef and drugs
 Image copyrightGETTY IMAGES
Image copyrightGETTY IMAGESUS lobby groups for agriculture and pharmaceutical firms want UK standards changed to be closer to those of the US in a post-Brexit trade deal.
The meat lobby wants the sale of growth hormone-fed beef, currently banned in the UK and EU, to be allowed in the UK.
The drugs company lobby wants changes to the NHS drugs approval process to allow it to buy more of US drugs.
They are also asking US officials – who will hold a hearing later – to seek lower tariffs on agricultural goods.
The farming groups say any deal should move away from EU standards, including rules governing genetically modified crops, antibiotics in meats, and pesticides and herbicides, such as glyphosate.
Technology groups are also setting out their wishlists for any pact. Companies in this sector are against the UK’s proposed digital tax.
The UK government has promised to look at ways of taxing US technology giants, such as Amazon and Google, which critics say do not pay their fair share of tax in the UK and therefore operate at an unfair advantage to physical companies.
‘Once-in-a-lifetime’ opportunity
The lobby groups’ priorities were outlined in more than 130 comments submitted to the office of the US Trade Representative.
The office solicited the feedback to help develop US goals as it prepares to start trade talks with the UK after Brexit.
It is hosting a hearing in Washington on Tuesday on the subject.
US companies – especially in the agricultural sector – said they hoped the UK would prove more flexible than the EU.
UK negotiations could represent “a once-in-a-lifetime opportunity”, the National Grain and Feed Association and North American Export Grain Association wrote.
The groups said a new deal could create a trans-Atlantic market “that can act as a bastion against the EU’s precautionary advances and its ongoing aggressive attempts to spread its influence around the globe”.
 Image copyrightGETTY IMAGES
Image copyrightGETTY IMAGESImage captionUS agricultural groups have long complained about EU rules
Here is a summary of goals for key sectors:
Agriculture
US business groups from the agricultural sector have been among the most vocal, amounting to nearly a third of all comments.
The groups, which as well as meat, drug and technology firms include producers of olive oil, wine, nuts, fruit, and dairy products, say they want to see the UK reduce tariffs on food products. They also want to limit geographic labelling rules, such as those that bar US companies from using terms such as Prosecco.
The Animal Health Institute, which produces animal antibiotics, was among several groups that said it would not support a deal that did not address demands by the US agricultural sector.
“We have noted with concern statements by certain UK officials indicating a desire to exclude the agricultural sector from the negotiation and an intention of maintaining regulatory harmonisation with the European Union,” it said.
“Should the UK adopt such policies, we see little basis for the negotiation of a bilateral trade agreement.”
Health
The pharmaceutical industry is also gearing up for negotiations to start.
PhRMA, which represents drug makers in the US such as AbbVie Merck and Novartis, said it wanted a deal to address the barriers to access it currently faces in the UK, pointing to items such as government price controls.
It heavily criticised the current NHS drug approval system, pointing to the cap on the price of drugs as too restrictive, and highlighting insufficient healthcare budgets and “rigid” national processes.
The organisation, as well as some other groups, are also hoping to secure patent protections for certain types of drugs for at least 12 years, among other demands.
Technology
US firms also want to bar a proposed UK tax on digital services and prohibit rules requiring that data be stored locally.
- Budget 2018: Who will pay the Digital Services Tax?
- US attacks UK plan for digital services tax on tech giants
There is also widespread support to push the UK raise the amount that triggers customs duties from £135 closer to the US level of $800 – more than £600.
Such a move would make it easier for small businesses to export to the UK, said companies including e-commerce site Etsy.
Many of the demands in the tech sector also surfaced during negotiations of the trade agreement between the US, Mexico and Canada.
Saturday January 26th 20019
US government workers and many of its agencies have been on strike since December 2018, the strike sanctions were lifted yesterday Friday January 25th 2019. During this strike testing US cattle for BSE was halted.
These cattle untested for mad cow disease have now entered the US human food and medicine chain. The steaks and mince from these cattle untested for BSE now reside on Amercian supermarket shelves. Some of these untested cattle will also have been exported.
As US government staff return to their jobs, does this mean the US Agriculture Deparment will recall all beef and beef products processed for human consumption during the strike? or will profit and the huge food and drug corporations come before the US publics/human health?
THe USA have over 89 million cattle and thousands of these will not have been tested for BSE during the government workers strike.
See below how lack of testing for BSE mad cow disease in one state was a result of the government shut down.
Kate Richer victim of human BSE New mum Sally victim of BSE
Sunday 16th December 2018
My Andrew was unlawfully killed by the human form of mad cow disease on this day 2007 at 9.25pm, he was just 24 years old. Those I name and shame on this website made many deliberate choices and decisions allowing BSE infected material to flood the human food and medicine chain. I have seen and re-printed on this website and in my book ‘Who killed my son?’ the many secret memos, letters and documents that show clearly that the British Beef/Agriculture/ Pharamaceutical industries and their exports meant more than human health and life.
These I name and shame are culpable in my only son Andrew Blacks unlawful death.
In the years since Andrew was killed, I have continued to battle the authorities and those responsible for Andrew’s death. All victims of human mad cow disease here in the UK and their families demand, deserve and want justice. The fight continues until all victims across the UK and globally see those culpable for the biggest health scandal in recent years are made accountable in a criminal court. All those individuals who I name are responsible for my Andrew’s unlawful death and so many others killed, thousands disabled and millions of us ‘at risk’ of developing human BSE. Those named and shamed should face lenghty jail sentences and financial punishement.
The pain of loosing my son Andrew to an avoidable and acquired diseased, never goes and time does not heal.
People ask me, ‘ you must miss Andrew so much’
I always reply, ‘Yes I do. But the worst is, ‘missing what my son is missing’
 Emma and Andrew in happier times
Emma and Andrew in happier times

My family of 3 before BSE struck
The thousands of sunrises, the sunsets, the laughter, the living, the loving the everything that is attached to being alive and just 24 years old, on the brink of so much life and potential. I miss the future Andrew would have had, the individuals he would have met, maybe married, the children he would have had, the 60 years plus of life he should and would have lived.’
This is what I miss more than anything…………………
Love always and forever to my number one and only son Andrew, till we meet again.
Love Mum xxxxx
And your little sister Emma, who at 28 years old is now older than her older brother.
Tuesday 27th November 2018
Mother dies after being ‘infected’ with cjd in the womb by her baby? See these news articles below regarding research by Danish Scientists who found that a father died of the inherited form of cjd. He had impregnated his wife who had a son, this child then infected his mother in the womb with cjd and she died of sporadic cjd. The son now 53 years old has symptoms of cjd.
Read Daily Mail article below.
Confused? so am I and the global public.
I feel this is a very odd case and points more at an envrironmental cause in which all the family were exposed to an infectious agent.
This agent then caused the various strains in the child and mother. Thed inherited form form of cjd can not transmitted to a mother or sexual partner, but according to this research the baby carried the inherited gene and then infected his own mother in the womb!
I wonder are all these forms merely another strain of vcjd the human form of BSE/Mad cow disease?
Also it raises questions regardging surrogacy and egg/sperm dontation, if as this research paper suggests cjd can be transmitted in the womb/via sperm.
https://www.nzherald.co.nz/lifestyle/news/article.cfm?c_id=6&objectid=12166780https://www.express.co.uk/news/science/1050654/health-news-dementia-pregnancy-creutzfeldt-jakob-diseasehttps://www.dailymail.co.uk/health/article-6429721/Woman-dies-rare-form-dementia-decades-catching-BABY-pregnant.htmlhttps://www.thesun.ie/news/3438306/mum-dies-after-catching-a-rare-form-of-dementia-from-her-baby/
Recent news on BBC TV october 2018
Daily Mail online
Woman ‘dies from a rare form of dementia’ decades after catching it from her own BABY while pregnant
- Infant inherited a gene from its father that made him produce toxin proteins
- Mother did not have the gene but died of the same disease 50 years later
- Cells from the foetus contained the proteins and traveled to its mother’s brain
A woman has died from a rare form of dementia decades after she is thought to have caught the disease from her own baby while pregnant.
Her husband died of sporadic Creutzfeldt-Jakob disease two decades ago – but her own genes were previously shown to be clear of the responsible mutation.
However, the unidentified woman, from Denmark, died of the same crippling disease as her late husband while in her seventies.
Her son, whose identity has also been withheld but is known to be 53 and a father himself, is now ‘showing symptoms’ of sporadic CJD.
A woman has died from a rare form of dementia decades after she is thought to have contracted the disease from her own baby while she was pregnant (stock)
Doctors now believe the son inherited the mutated gene responsible for the disease from his father, before passing it back to his mother while in the womb.
Cells from the foetus that contained the toxic proteins are thought to have traveled across the placenta into her bloodstream, before lodging in her brain.
The fatal condition causes irreversible brain damage, triggered by abnormal proteins known as prions, which gradually destroy brain cells.
The rare case was uncovered by a team of medics at the Danish Reference Centre for Prion Diseases in Copenhagen University Hospital.
The woman was diagnosed with sporadic CJD before the disorder was linked to her late husband or son.
Ausrine Areskeviciute, one of the medics who stumbled across the case, told The Times that it is a ‘very sad story’.
She said: ‘We already know that when a woman is pregnant cells from the baby travel across the placenta and travel around her body, lodging in various organs.
‘However, in this case the foetus carried the mutation for the misfolded proteins, and its cells may also have had misfolded proteins when they got into the mother’s body.’
Ms Areskeviciute added this may have triggered the process that led to her death years later.
The case of CJD, which is considered to be a type of dementia, was published in the Journal of Neuropathology & Experimental Neurology.
CJD, of which there are four main types, is a prion disease, which derives its name from ‘protein’ and ‘infectious’.
It is defined by proteins in the nervous system taking on an unusual shape, which then spread in a domino-like effect to cause lesions in the brain.
Some 85 per cent of cases occur randomly, while 10-15 per cent are inherited. In less than one per cent of incidences, CJD is acquired.
Mad cow disease is also a prion condition, which occurs when a person eats meat from cattle affected by a similar disease.
Sporadic CJD affects as little as one in a million people each year in the UK, NHS figures state.
This comes after research released earlier this year suggested prion diseases can be spread during operations via poorly-cleaned surgical equipment.
Monday 19th November 2018
Severely disabled girl, 19, and grandmother could lose home due to benefit cuts
Across all media today is the story of severely disabled Emily Lydon, born to Sally Evans in 2001 who was suffering at the time with the human form of mad cow disease. Sally at just 24 years old sadly died of human BSE 7 months after the birth of Emily.
New mother Sally Evans dying of human BSE with baby Emily
Emily is now 19 years old has been disabled from birth and is unable to walk, talk, eat, she shows all the signs of having the human form of mad cow disease. Because Emily is MV it may well have slowed down the progression of the lethal disease.
The UK government refuse to accept this diagnosis.
Emily is looked after by her devoted grandmother Jean Godfrey. I know Jean very well and have seen how Emily has grown over the years.
The UK government are now cutting the benefits to Emily which may mean Emily and Jean will lose their home.

Emily was placed under a legal injunction until she reached 18 years old, this meant that her grandmother Jean and no media could report on Emily’s plight and resulting disablement.
Now Emily is 19 years old, Jean can speak freely about her granddaughters disablement by Human BSE transmitted from her mother Sally, during pregnancy in the womb.
The UK government continue to silence all victims of vcjd and treat them appallingly. By lowering Emily’s benefits it will also lower Emily’s life expectancy.
Due to the devoted care of her grandmother Emily remains well. If benefits are cut this could seriously endanger Emilys’ health and well-being.
https://metro.co.uk/2018/11/18/severely-disabled-girl-19-and-grandmother-could-lose-home-due-to-benefit-cuts-8153594/?ito=article.desktop.share.top.email
THE METRO Lucy Middleton
A brain-damaged girl and her grandmother could be about to lose their home after their benefits were slashed by more than half as a result of the universal credit switch. Emily Lydon, 19, was born brain-damaged after he mum Sally Evans contracted the human form of mad cow disease bovine spongiform encephalopathy (BSE). Since her mother’s death when she was just seven months old, the teenager, who cannot speak, walk or feed herself, has been looked after by her grandmother Jean Godfrey, 68. Emily Lydon lives with her grandmother Jean Godfrey.
But now the pair have been told that their joint income of £720 a week, needed to pay for Emily’s 24-hour care and transport, is being cut down to just £342. ‘Government failures let mad cow disease into the human food chain, killing my daughter and brain-damaging my granddaughter,’ Ms Godfrey, of East Markham, Nottinghamshire, told The Sunday Times.
‘I’ve spent 20 years caring for Emily. Now these benefit cuts could make us homeless.’ Ms Evans was one of the first Brits to get variant Creutzfeldt-Jakob disease (vCJD) and was unknowingly developing the infection before she became pregnant with Emily in 1999. The degenerative disorder attacks the brain and is always fatal. The pair have had their benefits cut as a result of the switch to universal credit.Emily’s mother died after contracting mad cow disease
The disease was spread though cannibal cow-feeds, in which sick cows were killed, minced and fed back to the rest of the cattle, spreading the illness to other herds and eventually humans through the consumption of beef. It it thought around 25,000 Brits still carry the infection while 178 have died.
Ms Evans passed away in May 2000, aged 24, and since then Emily has been cared for by Ms Godfrey, who is her main carer. The teenager can’t speak or eat, is doubly incontinent and must be fed through a syringe that pumps food into her stomach. But despite also not being able to walk, Emily was called to a jobcentre in Retford for a ‘work capability assessment’ by the Department for Work and Pensions (DWP). Ms Godfrey fears that they will lose their house as a result of the cuts
After being reviewed by staff, she was awarded £58 a week in universal credit and had other benefits of £520 a week cut. Ms Godfrey and her granddaughter have now been left with just £342 a week, less than half of their previous allowance
The pair have since been offered an extra £150 by a civil servant after The Sunday Times contacted the DWP – but they will not restore Emily’s full benefits as she is now ‘an adult’. ‘We are sorry for some of the communication in this case,’ a spokesperson said. ‘Because Emily has left full-time education she is no longer eligible for child benefits. She now receives universal credit and a personal independence payment.’ But Ms Godfrey has called the concept of ‘adulthood’ for people with severe mental disabilities purely a discriminatory means to justify benefit cuts. ‘Even with the extra £150 our benefits are down by £200 a week under universal credit,’ she said. ‘It costs £150 a month for heating oil, so if we heat our house we can’t eat. I think we’ll still lose our home.’
Monday November 5th 2018
 Statue of cow near Bog Head Farm
Statue of cow near Bog Head Farm
BSE DIAGNOSED IN COW BOG HEAD FARM, LUMSDEN, ABERDEENSHIRE, SCOTLAND
The press statements from the NUF National Union of Farmers Communications Team and the reassuarance by Ministers in the Scottish Parliament are falsely reassuring. The cow diagnosed with BSE from Bog Head Farm, Lumsden in Abeerdeenshire was already dead when it was examined. So it was infectious/ill for weeks maybe months and only examined once it had died. BSE in cattle like human mad cow disease in individuals can have long incubation periods.
Would anyone from the Scottish Parliament or the NFU communications team eat a burger made from the surviving herd from Bog Head Farm? As tests are still on-going how can press statements and Ministers from the Scottish parliament tell the public that ‘there is no risk to human health’.
No Scientist, vet or expert can ever say ‘there is no risk to human health’ once a animal has been diagnosed with BSE.
BSE in cattle is never in isolation, what shops, supermarkets, schools did this farm supply? How many steaks, pies, burgers and meat products from Bog Head Farm, are now in UK shops? Being eaten by families across the Scotland and the UK?
DAILY MAIL 31st October 2018
Tests are being carried out on the carcasses of four cows destroyed at the Aberdeenshire farm where a case of BSE was found, MSPs have been told.
The animals were said to have been culled as a precaution earlier this week, with the carcasses taken to the south of Scotland for “sampling and disposal”.
The results of that analysis are expected to be available in a few days’ time.
It emerged in mid-October that an isolated case of BSE, known in full as bovine spongiform encephalopathy, had been found at a farm in the Huntly area.
A movement ban was immediately put in place at the farm as investigators worked to determine the source, and it emerged some other animals would need to be slaughtered purely as a precautionary basis.
Officials have stressed there is no risk to public health.
MSPs were updated after a case of BSE emerged earlier in October (David Cheskin/PA)
During a meeting of the Scottish Parliament’s Rural Economy and Connectivity Committee, Conservative MSP Peter Chapman sought an update on the investigations into whether the four other cows “are infected or not”.
Elinor Mitchell, director for agriculture and rural economy at the Scottish Government, responded: “The evaluations of the animals affected were completed on the farm on the 26th of October.
“Yesterday (Tuesday), the three cohort animals and the one offspring were culled on the farm.
“The carcasses have been transported for sampling and disposal to Dumfries.
“The screening results will be available at the end of this week.
“If any of them prove positive then those carcasses will be transported to the APHA (Animal and Plant Health Agency) Weybridge offices (in Surrey) for further testing.”
Mr Chapman expressed satisfaction with the development, saying: “I think that’s good. We’re absolutely sure, certain, that there are no other potential animals that could be infected.
“It’s just the immediate offspring of this particular cow and we know exactly where they are and they have now been taken out.”
Scottish Rural Economy Secretary Fergus Ewing said it was “hugely disappointing” to have the confirmed case of BSE and said it is right that investigations take time.
He said: “There is no risk to consumer health and the Scottish Government have activated plans to protect food safety and, of course, our valuable farming industry.”
He later spoke of the importance of the “very effective surveillance regime” in bringing the case to light.
Mr Ewing told MSPs: “We’ve got that. If we didn’t, we wouldn’t have detected the case and goodness knows what the consequences of that would have been.”
The farmer whose cow was found to have BSE previously said he had taken pride in doing everything correctly and it was “heartbreaking” to be told the dead animal had the disease after routine testing.
Scotland’s chief veterinary officer Sheila Voas has said she believes the disease was not transmitted, and occurred spontaneously in the affected animal.
Thursday 19th October 2018
Above : BBC report on BSE in beef herd Huntly, Aberdeenshire, Scotland 18th October 2018
What is the difference between a spontanous outbreak of BSE in cattle and Mad cow disease BSE in cattle? Millions of pounds lost to the beef, agriculture, food and drug industries. The cover-up continues, see below!
BSE FOUND IN BEEF HERD IN HUNTLY, ABERDEENSHIRE, SCOTLAND
—
Tuesday 9th October 2018
Pioneering new treatment for Sporadic cjd what about Human BSE vairant CJD? 1 in 2,000 of the UK population now ‘ carry or incubate the human form of mad cows disease’.
This is a huge breakthrough but, how many cases of sporadic cjd are really vcjd HUman BSE anyway?
Pioneering treatment for CJD to be given to a UCLH patient

CJD is a rare but devastating disease that causes brain damage and for which there is currently no treatment. It is always fatal and most patients sadly die within six weeks of diagnosis.
Researchers at the Medical Research Council (MRC) Prion Unit at University College London (UCL) have developed an antibody, called PRN100, for treating CJD. Laboratory testing of the antibody has been encouraging but it has not yet been used in patients.
UCLH is set to give the antibody to a patient for the first time in the world after a judge in the Court of Protection today confirmed that it is lawful and in the patient’s best interests to receive the unlicensed treatment.
UCLH’s chief executive Professor Marcel Levi said: “Creutzfeldt-Jakob disease (CJD) is a rare and cruel disease which rapidly destroys the brain, affecting memory, thinking, speech, balance, movement and behaviour.
“There is currently no cure or treatment for CJD. At present, caring for patients with CJD involves trying to use medicines to alleviate symptoms only but sadly, the disease always results in the rapid death of the patient.
“The court’s confirmation today is an important step forward in tackling this devastating illness.”
Professor Levi added: “UCLH is an innovative healthcare institution committed to ensuring our patients have access to the most cutting edge treatments available.”
Sporadic CJD, the most common form of the disease in humans, is caused when healthy proteins which exist normally in the human body become spontaneously misshapen and build up in the brain. These misshapen proteins, which are called prions, stick to other healthy proteins causing them to become misshapen too and the disease spreads through the brain.
Our immune system produces antibodies to fight infections which invade the body. However, as abnormal prions are made of one of the body’s own proteins, our immune system does not make antibodies to fight them.
Professor John Collinge, director of the MRC Prion Unit at UCL, who led the development of the PRN100 treatment, said: “The treatment is an artificially manufactured antibody which has been created in the laboratory.
“The antibody has been designed to bind tightly to normal proteins in the brain. The aim is to prevent abnormal prions from being able to attach themselves to healthy proteins, meaning that they cannot grow and cause devastation throughout the brain.
“As this is the first time this treatment has been used in humans we cannot predict what the outcome will be but laboratory testing has shown the potential to treat prion infection. A key issue will be whether a sufficient quantity of the drug is able to cross the blood brain barrier to reach the brain tissue where it needs to work.
“We will proceed with extreme caution in very tightly controlled conditions. A team of experts from a range of disciplines will make collective decisions in the best interests of the patient.”
The patient and their family expressed their wish to receive this treatment and supported UCLH’s court application.
The patient will initially receive the treatment by a drip into a vein in the arm. They will be monitored around the clock by a team of experts from UCLH.
We are preparing for a range of possible outcomes including the treatment having no measurable effect and the treatment slowing or halting the progression of the disease. The treatment is not expected to reverse any brain damage that has already occurred.
The patient may also experience side effects which could lead the clinical team to limit or halt the doses of the treatment given.
In order to provide this treatment to a patient, UCLH created an oversight group, independent of the MRC Prion Unit and treating clinicians. The group comprises world-leading experts from a range of disciplines and it has met regularly with lawyers and patient advocates from the charity Cure CJD Campaign. The group considered the numerous and complex clinical, safety, legal and ethical issues arising from the potential use of this unlicensed treatment for CJD.
We will await the response of the first patient to this treatment before we consider a second patient.
A Q&A about this treatment
For further information please visit our frequently asked questions section on Prion diseases and Creutzfeldt-Jakob disease (CJD) on our website.

Patient advocate: Colin Beatty, Cure CJD Campaign charity
Colin Beatty lost his wife, Annie (pictured right), to sporadic CJD in 2010. Annie was 70-years-old and the couple had been married for 40 years.
“The diagnosis was devastating. It was like a bomb had gone off in our family,” said Colin.
“Annie was a former nurse so she knew what CJD meant and she was very frightened.
“It was a very difficult time. We cried many tears but I felt like it was my job to keep the family strong.”
Colin, 75, from Dorset, said the illness made Annie vacant in the beginning. Then her speech became muddled and she would wander off without warning, which he said was terrifying.
“It was heartbreaking to watch Annie deteriorate.
“I nursed her at home initially but she became very difficult to care for so we had to admit her to a nursing home.”
Colin said if the PRN100 antibody had been available at the time, he would have wanted Annie to have had the opportunity to be treated with it.
“It’s true that the treatment carries potential risks, and the benefits are not yet certain, but without it, there is no hope. The only certainty with CJD is death.
“For us, the decision about whether or not to have the treatment would’ve been a no brainer.”
Following Annie’s death, Colin became involved with the Cure CJD Campaign charity. He has represented the charity on UCLH’s PRN100 oversight committee.
“I got to know the team at UCLH’s National Prion Clinic very well when Annie was ill.
“Since we lost Annie, I have been committed to helping the team find a cure for this terrible disease.
“I don’t want other people to experience what we went through.”
Colin and Annie met in 1967 while they were working on a cruise ship which travelled between New York and Bermuda. Annie was the ship’s nursing sister and Colin was an electrical engineer.
“I was besotted with Annie. She later told me that as soon as she saw me, she knew I was the man she wanted to marry.
“She was a bubbly, popular person who was always laughing.
“She was a wonderful and supportive wife. We did everything together – we were so close as a couple and as a family.”
Colin and Annie have two sons, Chris and Nick, and four granddaughters.
FRIDAY 21st September 2018
Mad cow disease/BSE found in USA, Florida herd. The USA has dropped its budget for BSE testing its 94 million cattle to just 20k a year.
Yet this animal with such minimal testing was found with BSE? See details of press release below 29th August 2018.
How many thousands of other cattle have BSE and are being allowed into the human food chain? As this particular infected animal was bought and sold several times, its impossible for the authorities to check its parents, siblings and other members of the herd that are probably also carrying/incubating the deadly brain wasting disease BSE. Those animals will already have gone to slaughter and entered the human food chain and will now be sitting on supermarkets/shops shelves across the US and abroad.
How many more innocent people will die at the altar of greed and corruption that is big business, government and the food and pharmaceutical industries?
USDA Announces Atypical Bovine Spongiform Encephalopathy Detection USDA 08/29/2018 10:00 AM EDT
USDA Announces Atypical Bovine Spongiform Encephalopathy Detection
USDA Animal and Plant Health Inspection Service sent this bulletin at 08/29/2018 10:00 AM EDT

Sunday 2nd September 2018
Today would have been my son Andrew’s birthday.
I will never again buy Andrew a birthday card declaring:
‘Happy Birthday Son!’
i will never be able to wish my son a ‘Happy Birthday’ ever again. I walk past the cards in gift shops with the words ‘ SON’ splashed all over their covers featuring cars, champagne, flowers. Multiple gifts arrayed depicting the wonders of a precious son’s ‘Birth Date’.
Inside I cry for all those seconds, minutes, days, weeks, months and years my son has lost. All the
‘Happy Birthday Son!’ cards I will never buy, give or share with my Andrew ever again.
The cakes I will not bake, buy and the gifts I will never choose.
There are no ‘birthday celebrations’ today, instead I will walk with Emma my daugher and Andrew’s younger sister to his graveside and put two bunches of flowers on top of the earth where he now lies.
This is the reality of loosing a child and loved one to Human BSE a needless, avoidable and unlawul death. So many lives lost and continue to be taken by Human BSE, a UK man made manufactured disease.
In the last week of August another cow has be reported with BSE in Florida, USA, how many other cows, domestic animals continue to get into the food chain, how many more people like my Andrew will die?
https://www.freshfromflorida.com/News-Events/Press-Releases/2018-Press-Releases/USDA-Confirms-Atypical-Bovine-Spongiform-Encephalopathy

Andrew (first left) with friends celebrating 2006
he was already starting to show symtoms of human BSE
Wednesday 22nd August 2018
The NEW SCIENTIST DISCUSSES A victim aged 36 years old, who became ill with vcjd in 2014 and how this unidentifed man was from the MV genetype. Its dismisses the death of Grant Goodwin in 2009 who was also MV and died of vcjd. Despite the UK govenment scientists and Professor John Collinge and the Tax payer funded CJD unit writing to the Goodwin family declaring that their son Grant had died aged 30 years old of vcjd and was from the MV gene group.
The Goodwins were warned by govenrment agencies not to speak to me as a member of the press and not to speak out about their son Grant’s diagnosis.
https://www.newscientist.com/article/2118418-many-more-people-could-still-die-from-mad-cow-disease-in-the-uk/

Grant Goodwin from Glasgow Scotland died of vcjd aged 30 MV genegroup
FRIDAY 17TH AUGUST 2018
My article about on-going grief was published online and in print in the Daily Mail.
Friends who cross the road to avoid you because you’ve lost a child: Grieving mother tells of her pain when sympathy ran out as people decided she should ‘move on’
Christine Lord’s son Andrew, died from Variant CJD ten years ago at age 24
She says people feel awkward and cringe when she talks about him
She says it seems there is a time limit on grief and people choose to avoid her
Christine experienced crushing isolation when she most needed unity
Father-of-five John, experienced odd reactions after his daughter Felicity died
He claims the atmosphere changed if he mentioned her even in passing
One counselor says bereaved parents feel expected to forget their child
By CHRISTINE LORD and KATHRYN KNIGHT FOR THE DAILY MAIL
On a recent holiday, a friendly couple sitting at the next breakfast table regaled me with stories of their grandchildren.
‘Do you have children?’ one asked. It’s a natural question, and one I expected — and, as always, I gave the only answer I could.
I told them I have a 28-year-old daughter and a son, who would have been 34. ‘Sadly, he died ten years ago,’ I added.
Then the conversation ground to an uncomfortable halt — and it wasn’t long before the couple left.

Andrew at School aged 6 years old
I should be used to it by now; since my beloved son Andrew passed away, I have learned just how deeply our society struggles to confront the reality of parental loss. Andrew was just 24 when, in 2007, his life was claimed by Variant CJD, the human form of what is colloquially known as mad cow disease.
Christine Lord (pictured right) revealed the struggles of coping with grief after the death of her son Andrew (pictured left) who died from Variant CJD at age 24 +4
Christine Lord (pictured right) revealed the struggles of coping with grief after the death of her son Andrew (pictured left) who died from Variant CJD at age 24
Watching my brave, beautiful first-born battle with this degenerative condition was the hardest thing I and his sister Emma have ever had to endure.
Andrew knew he was dying and, in his last week, asked: ‘Will you remember me?’
I sobbed as I promised that the pride I had in him was eternal and would endure until I took my last breath.
Yet I totally underestimated how difficult and off-putting others would find my attempts to keep that promise.

Christine and Andrew family holiday New York, Central Park, 2002
I don’t chatter on about Andrew needlessly, but when others talk about their children or parenting, I want to share my stories, too — to recall his smile, his jokes, his work successes. Yet, all too often, reactions to a mere mention of his name range from awkward silence to cringeing embarrassment.
While we have learned to openly discuss other uncomfortable realities — from cancer to mental illness — we still struggle to find the right way to handle the loss of a child, perhaps because it’s such an awful and terrifying event.

Christine Emma and Andrew in happier times
Yet many have suffered it. Official figures show that from 2010-16, between 8,600 and 9,800 people under 30 died each year. That means tens of thousands of newly bereaved mothers, fathers and siblings.
All of us will deal with our grief differently, but many find that the devastating ripples from their loss reach other areas, with marriage breakdown, depression and suicide bids all too common.
Andy Langford, a counsellor and chief operating officer for bereavement charity Cruse, says: ‘The death of a child is particularly devastating because both our future and part of our ancestry are severed at once. It feels entirely unnatural — we expect to bury our parents, and we feel we should die before our children.’
As a society, we’re not universally good at talking about grief anyway, but the death of a child compounds this as it is so difficult to accept. Sadly, bereaved parents often feel like they are expected to forget that child to avoid forcing other people to confront their own fears.’
Yet how could we possibly forget? Andrew will always be a part of my family, and a part of me.
Christine recalls her son Andrew (pictured age four) dying in her arms. She says the sympathy of others seemed to have an expiry date and many bereaved parents also feel an expectation to ¿move forward¿, to ¿forget¿, or to find ¿closure¿ after a year or two +4
Christine recalls her son Andrew (pictured age four) dying in her arms. She says the sympathy of others seemed to have an expiry date and many bereaved parents also feel an expectation to ‘move forward’, to ‘forget’, or to find ‘closure’ after a year or two
Andrew aged 21 years old San Diego USA
I raised him and his younger sister Emma as a single parent for most of his life. Until he fell ill my vibrant, kind son had everything going for him: a career he loved in the media and a great group of friends.
Then, towards the end of 2006, he started to suffer from weak muscles, anxiety and pain. Endless visits to the doctor proved inconclusive.
Desperate, I researched condition after condition and came to my own conclusions. I found seven young people in my area, Portsmouth, had died of Variant CJD, which is contracted by humans exposed to bovine spongiform encephalopathy (BSE) — mad cow disease. I was perplexed, as our family hadn’t eaten meat for many years due to health concerns. Yet the horrific catalogue of symptoms rang true for Andrew.
So, with trepidation, I raised my fears with doctors. Ten days later they were confirmed: Andrew had Variant CJD — we will likely never know how he contracted it — and was given six months to live.
It is impossible to fully describe the horror of watching my beautiful, physically fit son deteriorate before my eyes. vCJD punches hole after hole in the brain, robbing the body of its primary functions one by one. Andrew lost his sight, his hearing and his ability to move before finally, on a chilly December night, he died in my arms in his bed.
Andrew first day at school aged 4 years old
Both Emma — just 17 at the time — and I descended into the dark tunnel of extreme grief, compounded by the unbelievably cruel nature of Andrew’s death. It was senseless to me that something so simple as a meal had cut him off in his prime.
In the immediate aftermath there were times when I felt I might not physically survive. The mere act of taking another breath felt like a Herculean task.
And as ill-equipped as I felt to continue living while my child did not, I soon discovered that society was ill-equipped to deal with me, too.
Of course, in the early days, I received no end of welcome sympathy, practical help and listening ears. People did their best.
Quickly, though, I realised that often — not always but often — their sympathy came with an expiry date, in some cases soon after the funeral. It seemed there was a time limit on grief.
I’ve met many people who believe that after one year, or two, a bereaved parent should be able to ‘move forward’, to ‘forget’, or to find ‘closure’ — terms which make me shudder.
At the very least, they felt we should be able to neatly package our grief and give it a clear beginning, a middle and a final, accepting end.
Christine (pictured today) says each passing birthday and Christmas reminds her of a life missed out on. She lives in constant awareness of the experiences her son didn’t get to have +4
Christine (pictured today) says each passing birthday and Christmas reminds her of a life missed out on. She lives in constant awareness of the experiences her son didn’t get to have
It’s a message reinforced by endless television dramas: a death is quickly played out and followed by a weepy, emotional funeral, but then the plotlines quickly move on.
Yet, as grief counsellor Andy Langford makes clear, grief is timeless. ‘It’s not a case of moving on and the grief ending because we will always have a relationship with the person who has died.
‘What bereaved parents want more than anything is acknowledgement of that, for others to acknowledge their child’s identity, that he or she existed.’
Because, as I know all too horribly well, when you lose a child you deal with it for the rest of your life. My pain may not be as raw as it was, but my heart is still broken.
Contrary to common expectation, grief can expand with the years, instead of diminish — with each passing birthday and Christmas, each summer holiday crossed off on the calendar a reminder of a life missed out on.
When I most needed unity and proximity, my grief, and people’s inability to deal with it, led to crushing isolation – Christine Lord
Since my son’s death I have lived with a constant awareness of all he didn’t get to experience. To me, his memory is ever-present.
Yet with the passing of time others have become dismissive, less able to engage. Eager to forget the whole, horrible tragedy.
I have watched people I once called friends go out of their way to avoid me, crossing the road while walking their dog or, in the case of one ex-neighbour, turning his back on me in the local coffee shop where we once swapped pleasantries. While it makes me sad, I can understand it a little: I hold up a mirror to their worst fears, making them think about things they would rather not.
But the fact is that when I most needed unity and proximity, my grief, and people’s inability to deal with it, led to crushing isolation.
One close friend with children the same age refused even to visit once Andrew had been diagnosed. She said she ‘couldn’t face’ seeing him — as if I or anyone else wanted to see him like that. And aside from a bereavement card, she has not been in contact since. It was another aching loss to add to the one that had redefined my life.
Christine (pictured with Andrew as a child) says not telling the truth about her son when people ask about her children would feel like a betrayal of his memory +4
Christine (pictured with Andrew as a child) says not telling the truth about her son when people ask about her children would feel like a betrayal of his memory
Strangers bring their own troubling dynamic: it is only when you lose a child that you realise just how much adults bond by chatting about their offspring. Whether it is at the café counter, at a drinks party, or over that breakfast table on holiday, I brace myself as I await the inevitable question: ‘Do you have children?’
Not telling the truth would feel like a betrayal of Andrew’s memory, yet the truth brings responses from cliche to downright cruel.
I have lost count of the occasions I’ve been told ‘time is a great healer’, while in the latter category I’d put the mother of three healthy children and a grandmother six times over, who told me my son was ‘in a better place’, along with the neighbour who suggested I ‘get a dog’ to keep me company.
None, I am sure, intended to cause distress. I understand how difficult it is to know what to say in the face of profound grief.
I have often wondered if I should sanitise my feelings and choose, if not to lie, then to tell half-truths about Andrew
The irony is that so little is required to make us feel a little better: a simple touch on the arm and ‘I’m sorry’. Anything that acknowledges what we, the unenviable group united by losing a child, are feeling — even years after the initial loss.
Another member of this miserable group of bereaved parents is John, a father of five and successful businessman. He lost his youngest daughter Felicity, aged 21, following a car accident on a gap-year holiday.
Grief drove this confident, articulate man to profound despair and, as he resurfaced, he encountered another challenge that endures to this day.
‘I found that if I mentioned Felicity, even in passing, the atmosphere changed and became stilted and odd,’ he recalls.
‘Customers in my engineering business and even friends at social events would get embarrassed and didn’t know how to react. I’d start to feel guilty that somehow I had upset them, ruined their day or evening.’
It’s a guilt I recognise: I have often wondered if I should sanitise my feelings and choose, if not to lie, then to tell half-truths about Andrew.
That was John’s solution. He has found that the only way he can cope is to pretend his devastating loss hasn’t happened.
These days, when he meets new clients, he tells them he has four children, not five.
‘It made it easier,’ he tells me, head in hands. ‘I even took down a family photo of us all from my office wall. It became just too awkward. It’s as if Felicity has been wiped out.’
By denying her existence in order to spare other people’s discomfort, he feels he is losing her all over again.
IT consultant Nicholas, meanwhile, lost his 28-year-old son Will several years ago to cancer. His eyes fill with tears as he recalls attending a work conference and striking up a conversation with a stranger about their sons.
‘It was great to share, laugh and compare notes with this other father — it was a lovely relaxed evening,’ he recalls.
But when the stranger said how much he would love to meet Nicholas’s son, he was blindsided. ‘I drank my pint quickly and left as I couldn’t bear to say Will died three years ago. Bereaved parents are not supposed to laugh and chat about their late children.’
Yet how can we not? The fact is that talking about loss is essential for mental health — it certainly has been for mine. Andrew may be gone, but he remains a big part of my life and Emma’s and we talk about him a lot to one another.
If only others would, too. There is not even a word to sum up our plight — no ‘widow’ or ‘widower’ label to lend us dignity.
And yet, loss is an inevitable part of life, and one we will all suffer. So the next time a bereaved parent talks about their child, please don’t walk away. Instead, be brave. Listen, laugh and reminisce with them. They will be more grateful than you can know.
Who Killed My Son? by Christine Lord, is available from Amazon. Paperback £7.99, Kindle version £2.39.
Andrew aged 23
THURSDAY 16th August 2018
The Independant newspaper reports that Australia will be flooding the market post Brexit with meat products currently banned by the EU!
How Australia’s meat industry plans to flood post-Brexit Britain with products banned in EU
Exclusive: Campaigners and farmers concerned by removal of ‘technical barriers’ to trade with Australia that could cause influx of lower quality products August 5th 2018
https://www.independent.co.uk/news/uk/politics/brexit-trade-meat-banned-eu-australia-beef-liam-fox-dit-friends-of-the-earth-a8475006.html
Australian meat industry leaders are heavily lobbying their government to put pressure on Britain to accept products currently banned under EU law after Brexit.
Among the meat products suggested for export to the UK are hormone-treated beef and “burnt goat heads”.
Ministers from both countries met last week to discuss the future of their trading relationship, amid concerns that the Australian government could force the UK to lower food standards.
It comes as a petition supporting The Independent’s campaign for a Final Say on Brexit passed 570,000 signatures.
Trade minister Liam Fox has long mooted Australia as a key trading partner for the UK when it ceases to be part of the EU.
The Department for International Trade has stated it “will not lower food, animal welfare or environmental standards as part of any free trade agreement”.
“Maintaining them is the right thing to do for our consumers and maintains the UK’s world-renowned reputation for high-quality products,” a spokesperson told The Independent.
But Kierra Box, Brexit campaign lead at Friends of the Earth(FoE), said the government is “saying one thing but doing something completely different”.
“The government can continue to claim they are protecting our environment and health but in reality these promises are flimsy and unconvincing.”
Wednesday 15th August 2018
MONGOLIA REPORTS MORE CASES OF MAD COW DISEASE
TWO CASES IN AUGUST AND 15 CASE OF MAD COW DISEASE IN
Must soum of Khovd Province in the west in mid-May.
http://www.xinhuanet.com/english/2018-08/09/c_137378541.htm
Source: Xinhua| 2018-08-09 13:28:38|Editor: Chengcheng
ULAN BATOR, Aug. 9 (Xinhua) — Two cases of mad cow disease were found in Mongolia, local media reported on Thursday, citing the country’s Ministry of Food, Agriculture and Light Industry.
With more than 66 million livestock animals, Mongolia aims to raise meat exports tenfold in the coming years and to diversify its heavily mining-dependent economy.
But frequent outbreaks of livestock animal diseases such as mad cow disease and the foot-and-mouth disease have taken a toll on its meat exports. Most recently, 15 cases of mad cow disease were reported in Must soum of Khovd Province in the west in mid-May.

UK cattle still develop BSE
FRIDAY 20th July 2018
The research article below was published during a lot of other ‘media stories’. A great day to bury bad news. Brexit, World Cup Football, Trump. All of these stories were covered to excess whilst this health story that affects us all was virtually ignored. BSE CWD, human form of mad cow disease, is a pandemic in waiting!
As myself and others have suspected Chronic Wasting Disease in Elk/Moose/Reindeer/deer which is the equivalent of BSE in cattle can now convert human prions to related disease, ie Human BSE or the human form of mad cow disease.
It has been known for a long time that people who hunt and regularly eat deer or related animals across the USA and other countries have a higher rate of dementia or cjd type illness or disease. How many more people will die of the equivalent of BSE before safety measures are put in place? The cull all of the animals concerned including cattle that continue to die of BSE should be a priority, Not just a few random cattle, deer or herds. The disease both BSE and CWD is endemic in these types of domestic animals and animals that are eaten and are also used for medicinal purposes.
When Avian flu was diagnosed in Hong Kong every chicken and fowl was destoryed this stopped the disease in its tracks. Unfortuantely the west is motivated by money, greed and profit, with human and animal health at the bottom of the list. My son Andrew who died of vcjd aged 24 paid the ultimate price of that greed and corruption, corporate manslaughter by those named and shamed on www.justice4andy.com.
https://www.ed.ac.uk/clinical-brain-sciences/news/news-jul-dec-2018/cwd-prions-human-conversion
Chronic wasting disease prions can convert human prions into disease-associated form
Jul 2018: A team of CCBS researchers led by Marcelo Barria have published findings that prions that cause chronic wasting disease in deer and elk can convert human prions in a test tube to the disease-associated form.
Chronic wasting disease (CWD) is a contagious and fatal neurodegenerative disease and a serious animal health issue for deer and elk in North America. It might also be a public health issue. The recent discovery of CWD among free-ranging reindeer and moose in Europe prompted a group of CCBS researchers at the National CJD Research and Surveillance Unit to revisit the unresolved issue of whether CWD can spread from animals to humans, as can bovine spongiform encephalopathy (so-called mad cow disease).
Both diseases are caused by prions, misfolded protein particles that are detected in the neural tissue of infected animals. The researchers, funded by the Department of Health and Social Care and the Scottish Government, found that CWD prions from cervids (e.g., elk, white-tailed deer, and reindeer) in North America can convert the human brain prion protein in a test tube into the disease-associated form but that the efficiency of conversion is affected by variation in the cervid and human prion protein genes.
Given the similarity of North American cervids to those in Europe, the researchers underscore the need for a more comprehensive and thorough assessment of whether CWD can cross the species barrier and infect humans.
The findings have been published today in the journal Emerging Infectious Diseases. “Susceptibility of Human Prion Protein to Conversion by Chronic Wasting Disease Prions” by Marcelo A. Barria, Adriana Libori, Gordon Mitchell & Mark W. Head.
Related links
Emerging Infectious Diseases journal
Prion disease research at the Centre for Clinical Brain Sciences
National CJD Research and Surveillance Unit
This article was published on Jul 11, 2018
Christine filming for MBC
Friday 22nd June 2018
My interview with Mark Mardell for BBC, Radio4 World and One was broadcast today. The full interview as part of the 12 part series Brexit: A love story? is now avialable via the BBC podcast. My interview will be embedded on this website within the next week.
Below is a photo of me and Mark Mardell, talking about my son Andrew and the impact of BSE on my family and of course the UK public past, present. What will happen when we leave the EU and the de-regulation of food standards and safety measures?

Christine with Mark Mardell
FRIDAY 20th July 2018
Wednesday 30th May 2018
Large scale intensive beef farming in the UK, means cattle no longer eat pasture grass and are hemmed in a small area. This intensive farming in the 1980s and 1990s, created BSE and human BSE.
Greed and profit always comes before human and animal health. Read the investigation in the Guardian below. I wonder who is in charge and profits from the privately owned intensive farms? Supermarkets such as Waitrose, Lidl and the Co-Op buy meat from these beef farms.
The Guardian May 30th 2018
Revealed: industrial-scale beef farming comes to the UK
Investigation uncovers about a dozen intensive beef units, despite assurances that US-style practices would not happen here
Animals farmed is supported by
Animals farmedAbout this content
Andrew Wasley and Heather Kroeker
Tue 29 May 2018 15.00 BST Last modified on Wed 30 May 2018 08.59 BST
Some of the UK’s intensive units can hold up to 3000 cattle at a time. Photograph: Bureau of Investigative Journalism/Guardian
Thousands of British cattle reared for supermarket beef are being fattened in industrial-scale units where livestock have little or no access to pasture.
Research by the Guardian and the Bureau of Investigative Journalism has established that the UK is now home to a number of industrial-scale fattening units with herds of up to 3,000 cattle at a time being held in grassless pens for extended periods rather than being grazed or barn-reared.
Intensive beef farms, known as Concentrated Animal Feeding Operations (CAFOs) are commonplace in the US. But the practice of intensive beef farming in the UK has not previously been widely acknowledged – and the findings have sparked the latest clash over the future of British farming
The beef industry says that the scale of operations involved enables farmers to rear cattle efficiently and profitably, and ensure high welfare standards. But critics say there are welfare and environmental concerns around this style of farming, and believe that the farms are evidence of a wider intensification of the UK’s livestock sector which is not being sufficiently debated, and which may have an impact on small farmers.
In contrast to large intensive pig and poultry farms, industrial beef units do not require a government permit, and there are no official records held by DEFRA on how many intensive beef units are in operation.
But the Guardian and the Bureau has identified nearly a dozen operating across England, including at sites in Kent, Northamptonshire, Suffolk, Norfolk, Lincolnshire, Nottinghamshire and Derbyshire. The largest farms fatten up to 6,000 cattle a year.
A number of British supermarkets are among those found to be sourcing beef from UK intensive farms.
Drone footage and satellite images reveal how thousands of cattle are being kept at some sites in outdoor pens, known as corrals, sometimes surrounded by walls, fences or straw bales. Although the cattle will have spent time grazing in fields prior to fattening, some will be confined in pens for around a quarter of their lives, until they are slaughtered.
Supermarket demand is believed to be, at least in part, driving the trend. In addition, some smaller and medium-scale beef producers have struggled to farm profitably in recent years, with sometimes tight margins and fluctuating costs. Most of the units identified are believed to have grown incrementally, rather than setting up from scratch.
A number of retailers, including the Co-op, Lidl and Waitrose, are among those found to be sourcing beef from UK intensive industrial scale farms, most of which are privately owned but sell to beef processing companies, which in turn supply retailers.
Chris Mallon, director of the National Beef Association (NBA), the industry trade body, said the reason the largest units have come about was purely down to “efficiency”.
“What we’re talking about here is commercial production, for feeding people. It’s not niche market. A lot of this will be on supermarket shelves – that’s where it’s coming into its own. In the catering side as well, they’ll be doing it,” he said.
“One of the things we’ve seen over the years is supermarket domination of the beef trade. What they want is specification, size of cuts, size to fit certain packaging, size of roasts – this has all become incredibly important.”
But he cautioned that farms dedicated to fattening cattle had always been bigger than those rearing them, “so actually having higher concentration of feeding cattle on units [isn’t new].
“The difference is we’re getting some larger units now and that will be because of economies of scale … if you can give the people you’re supplying a constant supply of cattle that are in the right specification, that makes you more valuable. And that’s one of the reasons we’ve seen a move towards it.”
Dr Jude Capper, a livestock expert who has studied intensive beef units in the US and elsewhere said that due to economies of scale “it’s almost inevitable that a larger farm can produce a greater quantity of a more affordable product – we see this in almost all agricultural sectors globally, just as we do in other industries”.
“Cows belong on pasture,” according to Compassion in World Farming.
The Guardian and Bureau last year revealed that 800 poultry and pig “mega farms” or CAFOs have appeared in the British countryside in recent years, some housing more than a million chickens or about 20,000 pigs.
Following the revelations, the environment secretary, Michael Gove, pledged that Brexit would not be allowed to result in the spread of US-style agribusiness: “I do not want to see, and we will not have, US-style farming in this country,” he said in a parliamentary statement.
Although the number of beef units is tiny in comparison with intensive poultry or pig farms, the latest findings have further fuelled fears that the UK could be embracing industrial-scale practices.
Caroline Lucas, MP for Brighton Pavillion, said the farms were “gravely concerning” and that “with Britain hurtling towards Brexit, and with our animal and environmental protections facing an uncertain future, I’m worried that we could end up adopting more of this US-style agricultural practice”.
Richard Young, Policy Director at the Sustainable Food Trust, said: “Keeping large number of cattle together in intensive conditions removes all justification for rearing them and for consumers to eat red meat… More than two-thirds of UK farmland is under grass for sound environmental reasons and the major justifications for keeping cattle and eating red meat are that they produce high quality protein and healthy fats from land that is not suitable for growing crops.”
Young added that that smaller scale beef farmers might feel the impact, as larger farms were likely to be “more efficient in purely economic terms”, allowing the supermarkets “to drive down the retail price of beef below the price at which more traditional farmers can produce it. As a result they go out of business.”
Beef production in the UK typically involves three distinct stages – calf rearing, growing and fattening – with many farms specialising in one part of the rearing process. Cattle may move between a number of different farms during their lifecycle. (A smaller number of farms rear cattle from birth and keep them on the same farm until being sent to the abattoir.)
After spending time on pasture many cattle are moved to dedicated “finishing units” and are typically housed in barns or grazed whilst being fattened ahead of slaughter, often for around 6 months. Many are fed specialist diets designed to encourage weight gain.
But in the US, much beef fattening takes place in “feedlots” with cattle held in vast outdoor pens where the largest facilities confine up to 85,000 livestock. Such “feedlots” have proved controversial in the past, both because of their size and because many cattle were given hormones and antibiotics, sometimes to encourage rapid growth. (Such practices are not permitted in the UK).
Despite acknowledging the arrival of intensive beef farming in the UK, experts reject the notion that the British beef sector will see a wholesale shift towards farming on a US-scale.
In the US the rise of the CAFO has been paralleled by a fall in the number of small farmers.
“Are we likely to see huge – 100,000 head – feedlots? No. We don’t have the market, infrastructure or public demand for them,” said Capper. “However, could we make better use of male calves from dairy farms by rearing them for beef in feedlot-style operations, using feeds that we cannot [or] will not eat, such as by-products from human food crop production? Absolutely – some beef producers are already doing this.”
Caroline Lucas called for the system of permits to be tightened up, and said “the Government should be officially recording the number of feedlots rather than letting reporting slip through a loophole … we need a proper debate in this country over what kind of agriculture we want in the future.”
A spokesperson for DEFRA said that “beef farms are regulated in exactly the same way as any other farms”. But it later acknowledged that “Defra does not have a database of feedlot style units…The Cattle Tracing System can provide figures on the number of holdings split by premised type e.g. Agricultural Holding, Slaughterhouse, Market etc. and the number of animals registered to each. However, it does not hold any data in respect of the feeding practices on the holdings.”
Waitrose said of its own supplier: “Animal welfare is of the highest importance to us and a large farm does not equal poor animal welfare standards. The farm is run under a bespoke environmental management plan in conjunction with Natural England. All the cattle graze the marshes during the summer season then during the winter months, when the grass is dormant the cattle are bought back to the yard when the finishing/fattening cattle are housed in covered sheds. For clarification the length of grazing season is weather dependent, once the grass stops growing the cattle need to be yarded and fed a forage based ration in accordance with animal welfare and best practice.”
A spokesperson for the British Retail Consortium said: “Our members take their responsibilities to animal welfare very seriously and work closely with trusted suppliers so that high welfare standards are upheld. They have strict processes in place and will thoroughly investigate any evidence of non-conformity to ensure that any problems are immediately addressed.”
The reason that larger units have come about is down to efficiency, according to Chris Mallon, director of the National Beef Association.
The reason that larger units have come about is down to efficiency, according to Chris Mallon, director of the National Beef Association. Photograph: Bureau/Guardian
The Guardian approached several of the largest units but all declined to comment.
Some in the beef industry itself have expressed unease about the intensive farming system. Russ Carrington, of the Pasture Fed Livestock Association, said: “It is sad that the travel towards cheap, de-valued food has led to the removal of livestock from fields. There is a very different, more sustainable way of producing high quality beef which is also considerably healthier for humans to eat – 100% grass-fed and grain-free, which has lower total and saturated fat content, a better ratio of omega 3 to omega 6 fatty acids and more vitamins and minerals, which comes from the diverse pasture they eat.”
Pressure group Compassion In World Farming (CIWF) have raised concerns that some cattle held at in “feedlots” are kept in “high stocking densities” with little or no shelter or shade and “no dry ground to rest on.” The group says it believes “cows belong on pasture”.
 Christine and Andrew aged 18months 1985, just a few years before the first UK cow was officially recognised as dying of BSE. Though that was kept secret from the public by the UK Government and its ministers for a few more years.
Christine and Andrew aged 18months 1985, just a few years before the first UK cow was officially recognised as dying of BSE. Though that was kept secret from the public by the UK Government and its ministers for a few more years.
In response Dr Jude Capper said: “In my experience at feedlots all over the world, I’ve yet to see any welfare issues that are inherent to the system. If we are to assume that cattle must be able to graze to lead a ‘happy’ life, then confinement may be regarded as an issue. However, I’ve yet to see this being backed by [any evidence-base].”
“It’s almost inevitable that a larger farm can produce more a greater quantity of a more affordable product,” says Dr Jude Capper.
“It’s almost inevitable that a larger farm can produce more a greater quantity of a more affordable product,” says Dr Jude Capper. Photograph: Bureau/Guardian
Evidence compiled by the Bureau and Guardian suggests that most intensive beef farms appear to operate to high welfare standards.
Chris Mallon said: “Cattle actually will be very happy in [these systems]. Cattle in the wild don’t build nests for themselves or hide in caves, they’re an outdoor animal and I think we’ve got to remember that.”
Thursday 27th April 2018
https://www.youtube.com/watch?v=u08QddLT6yw
THURSDAY 27th April
Christine’s BBC INTERVIEW AND FEATURE PUBLISHED ‘ The silencing of bereaved parents!’
Lost For Words? The Silencing of Bereaved Parents
Lost For Words? The Silencing of Bereaved Parents
Portsmouth journalist and campaigner for justice for victims of vCJD (the human variant of ‘Mad Cows Disease’) Christine Lord recounts her experiences of losing a child and asks why society still struggles to acknowledge and address grieving parents.
Stage and TV actor Kim Cattrall – known for her role in ‘Sex in the City’ – told Radio 4’s Woman’s Hour in 2015 that she objected to terms like ‘childless’ to refer to women who have not had children.
“It’s the ‘less’ that is offensive: childless – it sounds like you’re less because you haven’t had a child,” she said.
Her objection got me thinking about my own situation and how language and wider society treat people like me. Like Kim, I don’t feel represented in the lexicon of parenthood because there are no words, titles or labels in the English language to describe my circumstances.
I am the mother of a dead child.
There. I have written those dreaded words. The worst nightmare of every loving parent/guardian, or caregiver. Stark prose from which most adults recoil, whether they are ‘child free’ or a parent.
My son Andrew was killed aged 24 years old in 2007. His sister Emma was just 17 when she lost her only sibling.
Yet Emma remains Andrew’s sister and I remain a mother of two.
We belong to a growing club whose membership runs into the tens of thousands in the UK. According to the Office of National Statistics, between 2010-16, between 8,600 and 9,800 young people under the age of 30 died annually in the UK (an average of 9,000 per year). This means tens of thousands of newly bereaved mothers and fathers every year. Hundreds of thousands across Europe and millions across the globe.
As a bereaved mother, qualified counsellor and journalist, I wanted to write about how it feels to be a parent of a dead child: how people’s sympathy often comes with an expiry date, and how we have a problem in our society if we cannot acknowledge and understand grief.
Bereaved parents are expected to neatly package our grief: to give it a clear beginning, middle and a final, accepting end, tears no longer shed, pain ceased and the dead child deleted as quickly as an unwanted email. At the same time, the catastrophic event of losing a child creates divisions within relationships – from close friends to work colleagues. In the media, parents of dead children are often written about as tragic humans, broken by tragedy.
How we treat grieving parents is important because it shows us how as a society we deal with – or hide from – our deepest fears, and the isolation this causes to those of us who have lived through those fears becoming real.
I buried my only son just a few days before Christmas on 21st December 2007. In the last week of his life Andrew asked me, ‘Will you remember me?’ I sobbed and assured him that I would always be so proud of him and would talk about him and his achievements until the day I died. Why wouldn’t I?
But in the months and years that followed, I learned that our society would often find my attempts to keep that promise difficult, embarassing, and off-putting. I still, proudly, declare that I am a mother of two children. In my experience, what to me is a simple fact has for others the power to perplex and shock.
I have discovered that many people view the death of a child as ‘taboo’; a subject that shouldn’t be talked about too often once the funeral has taken place. Part of this seems to be based on a perception that there is – or should be – a time limit on grief.
I’ve met many people who believe that after one year, or two has passed, a bereaved parent should be able to ‘move forward’, to ‘forget’,or to find some form of ‘closure’. All these terms have come to make me shudder, and to understand that our society does not like to address what life is like when you lose a child.
Contrary to this common expectation, the grief of bereaved parents is more likely to expand with the passing years, with each birthday, each Christmas and holiday. The life that should have been lived is ever present for us. Blinded by disbelief, we try and make sense of this unknown landscape, where we continue to live when our children are dead.
I still want to keep Andrew and his memory alive in my ongoing relationships. I want to talk about his job, his smile, his funny jokes. I don’t chatter on needlessly about Andrew, but when others talk about their children or parenting, I want to share stories about both of mine, too. This is not maudlin but a celebration. Andrew existed and he contributed to so many people’s lives and experiences. He will always be a part of my family, and a part of me.
In the early days after Andrew had died, I witnessed an array of responses. Sympathy, practical help and listening ears were welcome. But as time passed, people became dismissive, less able to engage.
‘He’s in a better place,’ I was told by a mum with three healthy kids and six grandchildren.
A neighbour suggested I ‘get a dog.’
Countless times I was told, ‘time heals.’
I’m not saying people mean to cause distress, I understand how difficult it is to know what to say in the face of tragedy and profound grief. But at the same time, to hear these remarks feels at worst, cruel, at best, thoughtless.
I spoke to John and Nicholas, two fathers who have also lost a child, and found similar experiences to my own.
John is 54, from Wimbledon, and a father of five. His youngest daughter, Felicity, died aged 21 after a car accident during a gap year holiday. He told me how he has to adjust his conversation in everyday life, so that he doesn’t upset other people.
‘After Felicity’s accident, I was totally numb for many years. I worked non-stop to try and ease the depression and shock. Meeting clients was and still is difficult.’
‘I am confident, articulate, I like socialising. But I found after Felicity’s death, if I mentioned my daughter even in passing, the atmosphere changed and became stilted and odd. Customers and even friends at social events would get embarrassed and didn’t know how to react. I then feel guilty that somehow I had upset them, ruined their day or evening.’
John put his head in his hands as he told me, ‘I don’t talk about Felicity at work anymore. I tell new clients I only have four kids, it made it easier. I even took down a family photo of us all from my office wall. It became just too awkward. It’s as if Felicity never existed, as if she has been wiped out.’
Nicholas, 48, is an IT consultant on the south coast. He raised Will as his own from the time Will was a toddler. Will died from cancer, aged 28. He excelled at sports and had just got engaged when he was diagnosed.
Nicholas told me. ‘Will was the centre of my world and I miss him so much. I would probably be a grandfather now if he was still alive.’
‘One night after a work conference in Scotland. I got chatting to a stranger in a bar. We both started to talk about our sons. It was great to share, laugh and compare notes with this other father. Of course we talked of other things and topics, it was a lovely relaxed evening. At the end of the evening the stranger said, ‘I’d really like to meet your boy, he sounds a great young man.’
With tears in his eyes, Nicholas told me, ‘I drank my pint quickly and left as I couldn’t bear to tell the stranger that Will had died three years ago. Bereaved parents are not supposed to laugh and chat away about their late children.’
I know exactly what John and Nicholas were talking about, it’s other people’s attitudes to our loss that can be shockingly painful.
It has been over ten years since Andrew was killed and no, the pain is not as raw as it was, but my heart is broken. It will remain shattered. There will never be a quick fix. Because my son is never coming home.
Losing a child is horrendous and terrifying, but it’s also something that as a society, we should try to learn from.
If a person has lost a husband or wife, the terms widow or widower lend a sense of dignity and significance. Would giving bereaved parents a definitive title offer the same respect and empathy?
In the decade since my Andrew died I still ache with longing, still get angry, still shed a tear. Yet people ask, astonished, ‘aren’t you over it yet?’ or tell me, ‘you need to move on’ as if I have failed in some way, or have just mis-laid a favourite handbag on a train.
Talking about my son has been essential for my mental health. All of us will suffer loss, death is an inevitable part of life. So the next time a bereaved mother, father, guardian, care giver talks about their lost child, please don’t walk away from difficult emotions and leave them alone with their grief.
Instead, be brave. Listen, comment, share, laugh and reminisce with them. It will be good for your mental health too.
Christine Lord’s book Who Killed My Son? is available from Amazon, with profits from the paperback/kindle versions going to her campaignwww.justice4andy.com, supporting families affected by BSE.
Her latest documentary about the food industry, Cows, Cash and Cover-ups? will be broadcast this year, and you can view the trailer below.
: https://vimeo.com/203115042
Friday 20TH April 2018
‘We detected a prion disease in dromedary camels (Camelus dromedarius) in Algeria.’
https://wwwnc.cdc.gov/eid/article/24/6/17-2007_article#comment
BSE, mad cow disease continues to spread its toxicity across the globe. People continue to die, develop or are disabled by human BSE/Prion Disease/vCJD. The disease has not gone away and continues to spread amongst the animal kingdom. The equivalent of BSE has recently been found in Camels in Algeria.
Camel meat and milk are everyday foods for many people across the globe.
Dolphins, cats, dogs, horses, deer, zoo animals,mink, have all been killed or are developing the equivalent of BSE. Which has spread to domestic animals as well as cattle including pigs.
With incubation periods upwards of 50 years in humans and many decades in animals, we continue to face a global ticking health time-bomb. One that continues to be ignored, hidden or dismissed by the very people, ministers and governments who are condoning and allowing BSE infected material to still feed humans and animals.
See below the latest research into the Camels in Algeria found to be infected with prion disease which is the equivalent of BSE.
Just last month March 2018, here in the UK, in Salisbury Hampshire, three people were nearly killed by the deadly use of a ‘nerve/ chemical agent’. There was rightly world wide disgust of the use of unlawful ‘chemical agents’. The UK government will now spend millions of pounds clearing and cleansing the areas affected.
Yet the UK and global governments continue to hide its head in the sand regarding the toxic and lethal BSE and its continual spread within animals and humans. UK and global blood donation supply is not tested for human BSE, people have died of vcjd/prion disease from receiving tainted blood. BSE and its human equivalent can take decades to develop and for humans or animals to become ill.
From camel meat to beef, animals in the UK and globally continue to die/develop BSE or its equivalent. The disease cannot be killed by cooking, boiling or searing, the disease can then can be passed on-wards to people by the food they eat, or vaccines, blood.

photo of Andrew aged 24 with his friend Becky. Just a few months before he died of human BSE.
The BSE toxic agent cannot be destroyed! It remains active for generations. BSE and its equivalent continues to be re-cycled within the human and animals population.
People in the UK and across the globe continue to die of vcjd the human form of mad cow disease. Yet these victims and families are kept away from the media, told to ‘ keep quiet’ and intimidated by government officials.
It appears the beef, pharmaceutical, and agriculture industries and corporations hold governments to ransom with their funding, and overflowing coffers and offers of cash.
Once again ‘profit always before human and animal health’.
‘Prions cause fatal and transmissible neurodegenerative diseases, including Creutzfeldt-Jakob disease in humans, scrapie in small ruminants, and bovine spongiform encephalopathy (BSE).
After the BSE epidemic, and the associated human infections, began in 1996 in the United Kingdom, general concerns have been raised about animal prions.
We detected a prion disease in dromedary camels (Camelus dromedarius) in Algeria.
https://wwwnc.cdc.gov/eid/article/24/6/17-2007_article#comment
Cows, Cash & Cover-ups? – Official Trailer on Vimeo
Cows, Cash & Cover-ups? Investigating vCJD – Official Trailer A documentary exploring Variant Creutzfeldt-Jakob Disease (vCJD), the human form of BSE (Mad
Cows, Cash & Cover-ups? – Official Trailer on Vimeo
Cows, Cash & Cover-ups? Investigating vCJD – Official Trailer A documentary exploring Variant Creutzfeldt-Jakob Disease (vCJD), the human form of BSE (Mad
Saturday 24th February 2018
Over 16 health and safety breaches in meat production every week in the UK. When will UK and global governments put human health before shareholders profits?
My son Andrew was unlawfully killed by the human form of BSE and UK man made deadly infection in cattle that then transferred to humans. Now one in 2,000 of the UK public carry or incubate human BSE, and with incubation periods upwards of 50 years many more could die or pass on this deadly brain disease via blood, operations and medical proceedures.
Se this Guardian Article which highlights the on-going risk to the public, meanwhile food corporations continue to profit at the expense of human and animal health.
Monday 12th February 2018
Read this article from the Star and Crescent online newspaper about my new documentary and the how much higher the stakes are regarding food and medicine safety post Brexit.
New Documentary Featuring Portsmouth Journalist Asks: Do We Know What’s in our Food?
Thursday 11th January 2018
President Trump continues to de-regulate the food industry in the USA, this means globally and especially post-Brexit the UK will be importing meat that is not thoroughly tested for BSE and also food and medicines imported from the US will not have strict regulations to eliminate mad cow disease. For Trump ‘profit it paramount’.
In Dec. 14 2017 press conference, Trump said the US government had taken 67 such deregulatory actions through Sept. 30 — with an annual savings to society of $570 million — and had imposed just three new regulations. Instead of two for one, the ratio was 22 to one, he said..
https://www.bloomberg.com/news/articles/2017-12-29/trump-stretches-meaning-of-deregulation-in-touting-achievements
The photo below was taken during my trip to South Korea. In 2008/9 after many years of South Korea banning US beef due to ‘mad cow disease’, a ‘cheap deal’ was done between the USA and South Korea. This deal made millions for the USA coffers and also big business in South Korea.
The ‘knock-down cheap’ US beef came and still comes from ageing US cattle, deemed ‘unfit for US public consumption’. These old herds of US cattle, very few tested for BSE continue to be sent to South Korea to feed its citizens and children. In South Korea school meals and national service is mandatory and the most infectious parts of these old, knackered US cows go to make meals for the South Korean school children/students and also South Korean military personnel.
This photo below was taken during the many peaceful demonstrations that the South Korean people including the elderly, students, children and families took part. These protests were to try to prevent the beef contract between the USA and South Korea. Unfortunately the US/South Korean beef contract was agreed and since then children, families, service personnel and hospital patients across South Korea have had to ingest ageing US beef in their daily meals.
I attended several of these peaceful demonstrations in Seoul, many led by Catholic priests and people of faith in 2008. The governments answer to ‘free speech’ was often brutal with unnecessary violence aimed at peaceful demonstrators. Many young students were blinded by water-cannon and elderly people thrown into prison, just because they attended these protests.
Many of those imprisoned talked about my Andrew, this website and my campaign.
Upwards of 50,000 people attended these demonstrations but their voices remained unheard. Unfortunately the deal was struck and USA cheap, ageing beef most at risk of BSE continues to flood into the South Korean food and medicine chain.
Big business and profit always comes before public and animal health.
Post Brexit and with President Trump shutting down agencies once funded to test US cattle for BSE and research into ‘human mad cow disease’ means the human food and medicine chain continues to process cattle and animals incubating or infectious with ‘mad cow disease’
It also means our blood supplies, vaccines and medicines continue to be exposed to humans carrying or infected with vcjd/prion disease/ human BSE.
The ticking health time-bomb that is human and animal BSE will continue to kill individuals and animals and with these de-regulation of health and safety rules another epidemic with human and animal victims becomes more and more of future possibility.
. 
South Korean peaceful demonstrators attacked by Police/Government Security forces
Saturday December 16th 2017
Ten years ago today at 9.25pm my only beautiful beloved son Andrew Black aged just 24 years old, was unlawfully killed by Human BSE/ Human mad cow disease. Now often quoted as vCJD or prion disease
Times does not heal, when a dearly loved child is killed needlessly through greed, corruption and cover-ups. When those responsible for his manslaughter have so far not faced criminal action or punishment.
I miss Andrew every day of my life, I miss what he is missing, the future he would and should have lived.
To quote Maya Angelou
‘People will forget what you said, people will forget what you did. But, people will never forget how you made them feel.’
My son Andrew made me feel sunshine, rainbows and the wonders of life through his eyes as a child and then as a young guy on the cusp of so much life, love and adventure. I miss his optimism, his laughter, his kindness and clarity. My Andrew was an old soul with much wisdom and compassion. He made me feel so happy.
I never forget or stop loving you Andrew, I will never stop fighting and searching for the truth. So that you and all victims of human BSE past, present and those unfortunately to come will get the justice you deserve and families the answers they need.

Andrew I send you hugs and love. I am still and always will be holding your hand……till we meet again…….
Mum x
Tuesday 28th November 2017
Latest research highlights the deadly consequences of BSE and how generations of our UK/global families remain at risk of human mad cow disease. This research shows how human BSE can be transmitted via skin.
http://www.telegraph.co.uk/science/2017/11/22/human-strain-mad-cow-disease-can-passed-via-skin/
Monday 27th November 2017
 Christine with Labour MP Stephen Morgan
Christine with Labour MP Stephen Morgan
I have just met with my Labour MP Stephen Morgan and am pleased that justice4andy has the backing of the Labour Party.
During our meeting Stephen Morgan and I discussed many of the deadly and on-going public health issues regarding human mad cow disease. Post BREXIT the stakes are even higher.
My new documentary ‘Cows cash and cover-ups?’ was discussed and I presented Stephen with a copy of my book, ‘Who killed my son?
i am currently finishing the final chapters of my new book, and with my feature film, Cows, cash and cover-ups? due for release in 2018, WATCH THIS SPACE!
YouTube: https://www.youtube.com/watch
Thursday 26th October 2017
I have just returned from visiting five countries across Europe. I like to say thank you to all the people and friends I made in Germany, Austria, Denmark, Sweden and Slovakia.
I conducted a lot of research for my latest book and the campaign.
Sky news and various media see below are covering the ‘Contaminated blood scandal’ in which thousands of people including many children across the UK were given lethal blood products condoned by government ministers. This sub standard blood were sourced from blood donors who were ill with a variety of transmissible diseases. These blood products/medicines were also sourced from blood donors who were either carrying or went on to develop vcjd, human mad cow disease.
Many of those implicated in the ‘Contaminated Blood Scandal’ are also named and shamed on this website and implicated in my Andrew’s unlawful death and all those affected by Human BSE. JOHN MAJOR, KENNETH CLARKE are in the frame …at the moment Kenneth Clarke has refused to comment to SKY news or other media questions.
A secret memo written in 1987 by John Moore clearly shows the dis-regard Thatchers government and her Ministers and officials showed for public health. The memo clearly states the scale of the problem with contaminated blood, and how many people were suffering and dying and also ways the government and its ministers could remove themselves from implication or responsibility.
These government memos were being written the same time that BSE and its lethal dangers to humans were also being kept secret from the UK and global community by the same ministers and officials in the Department of Health. Including Minister of Health Kenneth Clarke.
I wish all my colleagues and friends at ‘Contaminated Blood’ campaign the best with their fight for justice and I know that many of the same people/ministers/ officials culpable in the deaths of thousands due to ‘contaminated blood’ are also implicated in the BSE scandal and my Andrews unlawful death at 24 years old.

Andrews grave
Snip from SKY NEWS BROADCAST 26th October 2017
The document was unearthed by campaigner Jason Evans, whose father Jonathan was infected with both HIV and Hepatitis C and died in 1993, when his son was four.
The memo is a note of a proposal put to the Cabinet Home and Social Affairs Committee sub-committee on AIDS, a body that included some of the most high-profile ministers of the Margaret Thatcher Government including Willie Whitelaw, Norman Fowler, Douglas Hurd, Kenneth Clarke and future Prime Minister John Major.
QUOTE FROM MEMO ‘ IT WOULD BE CONSISTENT WITH THE POLICY OF NOT ACCEPTING ANY DIRECT RESPONSIBILITY FOR DAMAGE CAUSED IN THIS WAY’.
The meeting was convened to discuss the fall-out from the unfolding contaminated blood scandal on November 4, 1987, a day before the Haemophilia society was due to lobby MPs in Parliament.
By 1987 it was clear that thousands of people had been infected and were dying, and in the memo Mr Moore acknowledged the scale of the problem.
Saturday 2nd September 2017
Today would have been my only son Andrew’s 34th birthday.
I can’t imagine how he would look or be as a mature man. The life he should have led, the relationships he would have forged, the wonderful career he would have had in the media, the friends he would have made, the children and grandchildren with whom he may have been blessed. All those days, nights, months and years he has lost. All those holidays, family celebrations, he has missed.
The empty seat at the dinner table will never be filled, there is void in our family that grows bigger with the passing years.
Andrew far left with friends

Andrew (centre holdiing a bottle) celebrating his 23rd Birthday.
Forever Andrew will be a young guy in his early twenties, dying far too soon and young.
Today I will walk to the cemetery and place flowers on his grave. A journey I have made every week for ten years. The cemetery is a harsh and uncompromising place for parents who tend their children’s graves.
Time does not heal and until those responsible ( many named and shamed on this website) are punished for stealing my son’s life and future, there is no healing for me or any of those victims and families who have been affected by human BSE/ vcjd/cjd/ prion disease, the human form of mad cow disease.

Andrew aged 22 on his way to a shift at TalkSPORT National Radio, London
WEDNESDAY 23rd August 2017

Christine with translator Sean outside Korean Assembly. Seoul.Cheap USA Beef untested for BSE heading for South Korea. Beef seen as ‘unfit’ for American citizens
TUESDAY 1st August 2017
The research below highlights how people suffering from vCJD the Human form of BSE have passed the diseased on-wards through blood and medical procedures. This research found that many other tissues and parts of the body contain the rogue prions that cause human mad cow disease which are infectious and could have be a danger during surgery.
As this research states we need a individual blood test for vcjd so that all patients before hospital procedures are screened and all blood donors are screened for the human form of mad cow disease.
The consequences of BSE remains a lethal threat for millions of people across the globe and generations to come. A blood screening test for vcjd would stop the re cycling of this deadly disease within our global blood supply and during hospital procedures.
The UK Department of Health continues to with hold the facilities to implement a blood test for vcjd as it knows the legal implications when 1 in 2,000 people could be carrying of incubating the human form of mad cow disease.
All those named and shamed on this website would face criminal proceedings and the ‘establishment’ would be rocked to its core. This is why a blood test for vcjd will continued to be blocked by the UK DOH.
Volume 23, Number 6—June 2017 Synopsis
Research
Distribution and Quantitative Estimates of Variant Creutzfeldt-Jakob Disease Prions in Tissues of Clinical and Asymptomatic Patients
Jean Y. Douet, Caroline Lacroux, Naima Aron, Mark W. Head, Séverine Lugan, Cécile Tillier, Alvina Huor, Hervé Cassard, Mark Arnold, Vincent Beringue, James W. Ironside, and Olivier Andréoletti
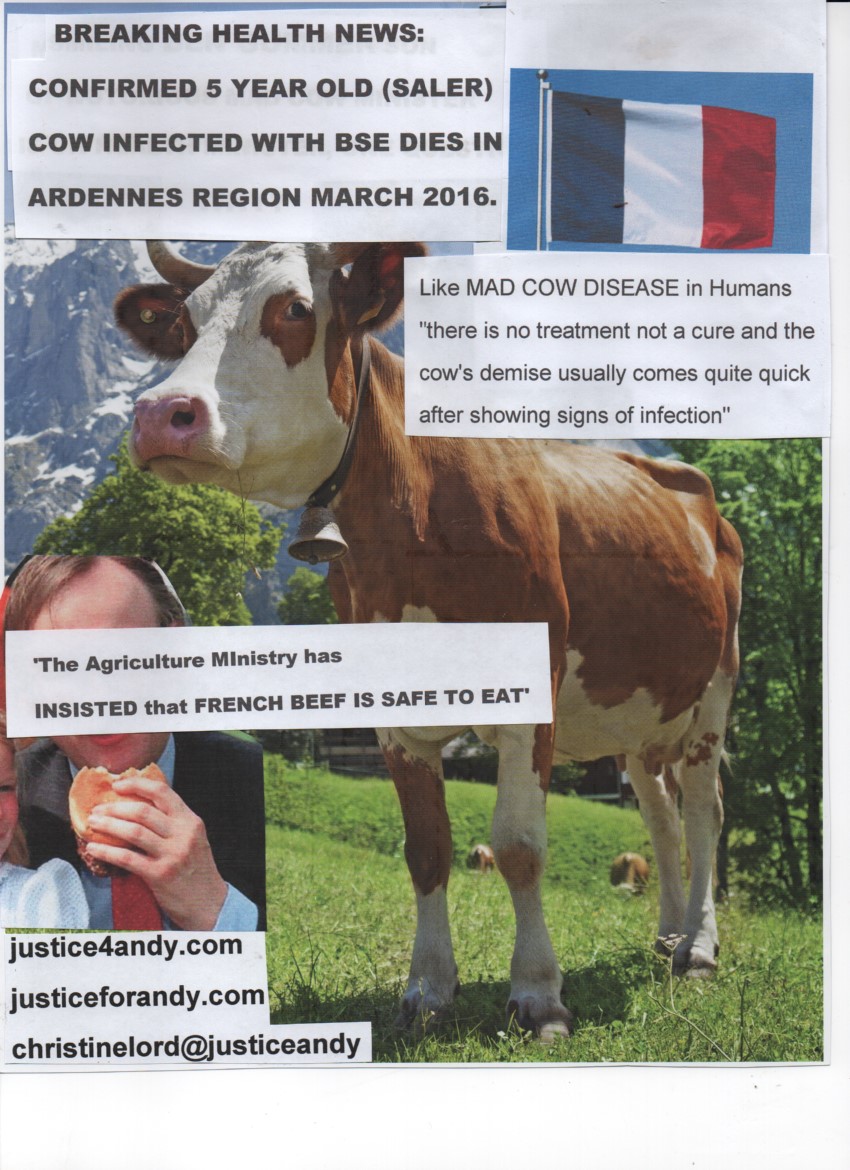
dementia link to human BSE
Comments to Author Author affiliations: Institut National de la Recherche Agronomique, Toulouse, France (J.Y. Douet, C. Lacroux, N. Aron, S. Lugan, C. Tillier, A. Huor, H. Cassard, O. Andréoletti); University of Edinburgh, Edinburgh, Scotland, UK (M.W. Head, J.W. Ironside); Animal and Plant Health Agency, Loughborough, UK (M. Arnold); Institut National de la Recherche Agronomique, Jouy-en-Josas, France (V. Beringue) Suggested citation for this article
Abstract
In the United-Kingdom, ?1 of 2,000 persons could be infected with variant Creutzfeldt-Jakob disease (vCJD). Therefore, risk of transmission of vCJD by medical procedures remains a major concern for public health authorities. In this study, we used in vitro amplification of prions by protein misfolding cyclic amplification (PMCA) to estimate distribution and level of the vCJD agent in 21 tissues from 4 patients who died of clinical vCJD and from 1 asymptomatic person with vCJD. PMCA identified major levels of vCJD prions in a range of tissues, including liver, salivary gland, kidney, lung, and bone marrow. Bioassays confirmed that the quantitative estimate of levels of vCJD prion accumulation provided by PMCA are indicative of vCJD infectivity levels in tissues. Findings provide critical data for the design of measures to minimize risk for iatrogenic transmission of vCJD
Andrew aged 23 loosing weight becoming ill with vcjd
Discussion
Most previous studies with tissue from vCJD patients have failed to identify consistent accumulation of the vCJD agent outside the nervous and lymphoreticular systems. However, data obtained in this study clearly demonstrate the presence of vCJD prions in a wide and unexpected variety of peripheral tissues.
Natural scrapie and experimental BSE in sheep are 2 models of orally transmitted prion diseases (24,25). In both diseases, the agent accumulates in the lymphoreticular system and the enteric nervous system during the early preclinical phase of the incubation period. Moreover, an early and persistent prionemia is observed in asymptomatic infected animals (26,27). These features were also observed in vCJD in humans and in view of the likely origin of vCJD (oral exposure to BSE agent), these similarities have led to a consensus that BSE and scrapie in sheep and vCJD in human have a common pathogenesis (28).
Although vCJD prions in a variety tissues, such as bone marrow, kidney, salivary gland, skeletal muscle, pancreas, liver, or heart, might be surprising, each of these tissue has already been demonstrated to accumulate prion infectivity or abnormal prion protein in TSE-infected sheep (29–33). Because low levels of infectivity have been reported in blood fractions from a vCJD-affected patient, such widespread tissue positivity might be derived from residual blood, rather than from the solid tissue in these samples (16). However, this proposal seems unlikely because in whole blood PMCA amplification inhibitors preclude detection of endogenous vCJD agent by this method (11,34–36).
 Andrew having fun as a toddler
Andrew having fun as a toddler
The patient in our study who was infected with a prion containing PRNP gene codon 129 Met/Val is 1 of only 2 identified vCJD agent–infected persons known to have died of other causes before onset clinical symptoms of vCJD, and the only person who provided consent to sample autopsy tissues for research. For this patient, all previous investigations did not detect abnormal prion protein or infectivity in the brain (12,37). The negative PMCA results we obtained for cerebral cortex, dorsal root ganglia, and trigeminal ganglia tissue from this patient are consistent with a lack of central nervous system involvement at the time of death. However, PMCA seeding activity in the pituitary gland was surprising in this instance.
The presence of abnormal prion protein accumulation in the pituitary gland and other circumventricular organs before deposition of PrPres in surrounding brain has been reported in TSE-infected sheep (38). However, this phenomenon in animals does not represent the main route for neuroinvasion and is a probable consequence of hematogenous dissemination of the TSE agent through the fenestrated capillary system of the circumventricular organs, which is substantially more permeable than the other capillaries in the brain (blood–brain barrier). Therefore, this finding might be a consequence of the hematogenous route of secondary vCJD in this person (by transfusion of packed erythrocytes from a vCJD-infected donor), in contrast to the oral route of infection in primary clinical vCJD cases (12).
Andrew (centre sitting down) aged 23 one year before he died of vcjd
vCJD prions were detected in certain peripheral tissues from the patients infected with a prion containing the PRNP gene codon 129 Met/Val. Although distribution of vCJD seeding activity in lymphoreticular tissues was similar to that observed for symptomatic vCJD patients, several tissues that were positive in clinically affected patients were negative in this heterozygous asymptomatic person. These findings suggest that involvement of some peripheral tissues might occur at a later stage in the incubation period than others, or that they could involve recirculation of the agent from the central nervous system (i.e., centrifugal spread in a late state). However, we cannot discount the possibility that that these differences in tissue distribution are caused by the hematogenous route of infection in this person (as opposed to the probable oral route in patients with clinical vCJD) or the difference between the PRNP gene codon 129 genotype of the asymptomatic vCJD–affected person (PRNP gene codon 129 Met/Val) and persons with clinical vCJD (PRNP gene codon 129 Met/Met).
Irrespective of the actual explanation for these differences, the presence of vCJD agent in peripheral tissues of patients during preclinical and clinical stage of the disease indicates the potential for iatrogenic transmission of this fatal neurologic condition by surgical procedures. Furthermore, this finding shows that, for certain peripheral tissues, a level of infectivity equivalent to an end stage titer (and attendant risk) is reached at a preclinical stage.

Several hundred cases of iatrogenic CJD have been reported worldwide. These cases appear to result from transmission of sporadic CJD, and most cases have occurred in recipients of human dura mater grafts or after administration of human growth hormone extracted from cadaveric pituitaries (39). Although in sporadic CJD the distribution of the agent is largely restricted to the nervous system (central and peripheral), the wide distribution of the vCJD agent in the asymptomatic infected patient we report might serve to increase the range of medical procedures, including dentistry, organ transplant, and surgery involving nondisposable equipment, that might result in iatrogenic transmission of vCJD (40–43).
Nevertheless, >20 years after identification of the first vCJD patients, only 5 cases that are a probable consequence of iatrogenic vCJD transmission are known, all in the United Kingdom and associated with blood and blood products. These cases were caused by transfusion of non–leukocyte-depleted erythrocyte concentrates or by treatment involving large amounts of pooled plasma from the United Kingdom that were known to include donations from persons who later showed development of vCJD (12,44–46).
None of the 220 other vCJD cases identified worldwide have been linked to any other medical or dental procedure. Whereas this fact is reassuring, it would be unwise to disregard the threat that vCJD still poses for public health. Despite the relatively low number (n = 178) of vCJD clinical cases observed in the United Kingdom, the most recent epidemiologic studies indicate that ?1 of 2,000 persons in the United Kingdom could be infected with the vCJD agent (as indicated by the presence of abnormal prion protein detected by immunohistochemical analysis of lymphoid follicles in the appendix). Each asymptomatic vCJD-infected person represents a potential source of secondary infection. The data in our report offer an opportunity for refining measures that were implemented in many countries to limit the risk for vCJD iatrogenic transmission. The apparent concordance between PMCA biochemical and infectivity bioassay data, and the higher analytical sensitivity of PMCA, suggest that future research need not rely exclusively on time-consuming and costly animal bioassay.
Our results indicate the need for vCJD screening assays. After more than a decade of effort, several vCJD blood detection tests have reached a stage in their development that could enable their evaluation as screening or confirmatory assays (11,47,48). In particular, there is now a strong case for use of PMCA in a highly sensitive and specific blood test for vCJD, as indicated by our previous studies (11,16) and studies by Bougard et al. (35) and Concha-Marambio et al. (36). The relationship shown here between PrPres amplification by PMCA and detection of infectivity by bioassay indicates that PMCA seeding activity is a good surrogate marker of infectivity and could provide a sound basis for a vCJD blood test for use with blood or tissue donors.
Dr. Douet is a research scientist and assistant lecturer in ophthalmology at the National Veterinary School of Toulouse, Toulouse, France. His primary research interests are the pathogenesis of the prion disease with special emphasis on the iatrogenic risk of transmission.
Acknowledgment
Andrew as a baby just after having vaccines which I didn’t know were made from BSE infected cattle
This study was supported in part by the Department of Health Policy Research Programme and the Scottish Government. The National CJD Research and Surveillance Unit is supported by the Policy Research Program of the Department of Health and the Scottish Government (DH121/5061). The Edinburgh Brain Bank is supported by the Medical Research Council (MRC grant G0900580). The Unité Mixte de Recherche 1225, Ecole Nationale Vétérinaire de Toulouse was supported by the European Union FEDER/INTERREG (EFA282/13 TRANSPRION), the Institut National de la Recherche Agronomique Institut Carnot en Santé Animale, and an Agence Nationale Recherche grant (Unmasking Blood Prions; ANR-15-CE18-0028).
https://wwwnc.cdc.gov/eid/article/23/6/16-1734_article
WEDNESDAY 7th JUNE 2017
Chronic wasting disease or CWD is the equivalent of BSE in cattle and human mad cow disease/vCJD in people. CWD is killing deer, elk and animals that are hunted and are eaten by individuals and groups across the USA and Canada.
CWD in deer herds is the equivalent of BSE in cattle, and has the same lethal consequences to the animals and also to humans that eat or ingest infected meat from deer/animals suffering from CWD.
There have been many cases in the USA/Canada of people who hunt or have eaten deer developing CJD or dementia type disease. These cases have been dismissed by the authorities as being spontaneous and nothing to do with the individuals close proximity or having ingested meat from deer. The families of those killed by CJD/dementia type disease, who have been active hunters for many years insist that the symptoms suffered by their loved ones are exactly the same as my Andrew’s symptoms and other victims of vCJD. Both BSE and CWD are prion diseases and can have long incubation periods. All of these bereaved families concerns have been dismissed by the authorities.
Hunting of deer across the USA and Canada is a huge sporting activity with deer meat prized in many communities. There would be huge financial and legal implications if links were made between CWD in Canadian and USA deer herds and vCJD within the deer hunting community.
In the White Paper below experts highlight the ticking health time-bomb that CWD poses for deer/elk herds across the USA/Canada and also its deadly risk to humans. As many deer in the USA and Canada and across the globe are wild this also has huge implications for other wildlife and of course agriculture.
Most recently in the USA a deer herd was found to have CWD, the animals who were chronically diseased were destroyed and meat from the rest of the herd was distributed to ‘deprived people in the area’. As experts know, animals can be infectious with the lethal prions that cause vCJD in humans but be symptom free.
This is appalling as it means those poorer people are being allowed to eat meat from a herd infected with CWD, meat that is not deemed fit/safe enough to feed richer and more prosperous people in society.
So are these poorer folks being experimented upon to see how many of them develop vCJD in the next decades? In the same way that Margaret Thatcher and her government allowed BSE infected material to feed UK children in their free school meals and also vaccines made from BSE infected herds? Is this why so many younger people then died of vCJD in the UK and continue to die?
THE COVER UP CONTINUES.
WHITE PAPER
CHRONIC WASTING DISEASE CWD TSE PRION ZOONOSIS ZOONOTIC INSIDIOUS AND DIRE CONSEQUENCES AHEAD
Alliance for Public Wildlife Living Legacy White Paper
The Challenge of CWD: Insidious and Dire Only immediate action will avoid catastrophic outcomes
Valerius Geist, Professor Emeritus, University of Calgary David Clausen, (former) Chair, Wisconsin Natural Resources Board Vince Crichton, (former) Co-Chair, Canada’s National Wildlife Disease Strategy Darrel Rowledge, Director, Alliance for Public Wildlife
Download this White Paper Download this white paper and other related publications at www.apwildlife.org/publications For more information To order copies of this white paper or receive information about other related publications, please contact Alliance for Public Wildlife at info@apwildlife.org
CWD is now deemed to be the largest-ever mass of infectious prions in global history, and experts sum up the threat (to wildlife, agriculture, our economies, and potentially to human health) in two words: “insidious and dire.” Current policy and apathy toward the levels of CWD consumption by people has been described as “one of the most outrageous human susceptibility experiments in history.
We have a problem. A big problem. Chronic Wasting Disease (CWD), a sister to BSE or ‘mad cow,’ is threatening our deer and elk. Unfortunately, CWD has broad implications. Without immediate action, we are heading for worst cases outcomes that include severe population impacts, extinctions, crashing economies, and, although unlikely, potential transfers of CWD to people.
Chronic Wasting Disease is an incurable, always fatal degeneration of the brain. Technically, it’s a Transmissible Spongiform Encephalopathy (TSE), but there are a number of quite different versions, depending on species. They include in humans kuru and fatal familial insomnia, as well as some with even more unpronounceable names, such as the dreadful human Creutzfeldt-Jakob Disease (CJD) and Gerstmann–Sträussler–Scheinker Disease (GSS). The largest TSE epidemics have been in domestic or captive animals: such as Scrapie in domestic sheep, Bovine Spongiform Encephalopathy (BSE), or so-called ‘mad cow’ disease, Transmissible Mink Encephalopathy (TME) on mink farms, and CWD in captive deer and elk.
CWD emerged as a particular nasty variant, because it can be transmitted by body fluids of infected animals (urine, feces, and saliva). Unlike BSE, CWD is highly contagious and can spread to and through wild ungulate herds. The infective agents are mis-folded proteins called prions; they are virtually indestructible, can persist in the environment, and tiny quantities can transmit the disease. Prion diseases have repeatedly jumped species barriers—most alarmingly in the United Kingdom, when BSE-infected beef killed 229 people.

As CWD spread, naturally and through trade, the U.S. in 2001 officially declared a “State of Emergency.” Every factor has since gotten worse. It has now been confirmed in 24 US states, 3 Canadian provinces, South Korea, and recently in Norway. Field studies are confirming potentially severe impacts on wildlife populations. So far no transmission to humans has been documented, but the risk is not zero. Non-human primates and transgenic (humanized) mice have been infected. In many jurisdictions, a lack of awareness and availability of free, rapid, and convenient testing of harvested deer has led to significant level of human exposure. Estimates show 7,000 to 15,000 CWD-infected animals are being consumed by hunter families every year, and this number continuing to rise by as much as 20% per year. The combination of threats is sobering. CWD has been shown to persist and remain infectious in the environment, including in clay-based soils that can dramatically increase infectivity (up to 680 times). Decomposing carcasses create contaminated “super-sites.” Prions are extremely resilient, known to resist disinfectants, alcohol, formaldehyde, detergents, protein enzymes, desiccation, radiation, freezing, and incineration >1100°F. Facilities infected with CWD have resisted all efforts at removing the infective agent. Canadian officials report that even on premises thought to be very low risk, restocking with healthy animals led to a 50% re-occurrence of CWD.
Transmission occurs animal to animal, soil to animal, mother-to-offspring, and from exposed plants or other surfaces including tools or surgical instruments (even autoclaving is ineffective). Now there is evidence the infective agent is taken up via the root systems of plants growing in contaminated soils, with transfer to stems and leaves. These were shown to be infective via inter-cerebral injection (oral tests are ongoing).
Executive Summary
Left unchecked, the prospects for wildlife are bleak. CWD has clear population impacts; some models suggest extinction. Disproportionate impact on mature males carries implications for hunters and wildlife economies let alone populations. Still more bad news: Efforts for vaccines have failed, and evolutionary or adaptive salvation is unlikely and would be too late in any case. CWD is now deemed to be the largest-ever mass of infectious prions in global history, and experts sum up the threat (to wildlife, agriculture, our economies, and potentially to human health) in two words: “insidious and dire.” Current policy and apathy toward the levels of CWD consumption by people has been described as “one of the most outrageous human susceptibility experiments in history.”
The good news
There is, of course, much more—but we need to get to the good news: There is hope, beginning with the fact that CWD is relatively new—not a long-standing or indigenous disease of our wildlife. The vast majority of our herds are still disease-free. We have considerable expertise, leading-edge technologies, and the benefit of experience. We faced a crisis on this scale once before, almost exactly a century ago, when the very existence of wildlife on this continent was threatened by the severest of over-exploitation. Hunters and conservation organizations led the efforts to avert disaster. With the courage and foresight of presidents and prime ministers enlisting the best and ablest on both sides of the US/Canada border to enact science-based policies, they turned our greatest tragedy into a ‘triumph of the commons.’ Anchored in the public trust doctrine, and now recognized as the North American Model of Wildlife Conservation, it replenished an entire continent with wildlife.
We need, today, nothing less than a similar effort to manage the Chronic Wasting Disease crisis. We have the benefit of experience and principles for success. Following the Roosevelt Doctrine, the same concerned hunter and conservation organizations must once again be the standard-bearers of principled, science-and evidence-based leadership in wildlife conservation. We must be relentless in following the leading science and scholarship, tracking the evidence, and engaging in comprehensive analysis to foresee the implications. We understand how policies affect the spread of diseases, as documented in the scientific and historical record summarized below. This threat is dire, and immediate action is warranted.
While details and methods must be guided by science and evidence, there is significant agreement on critical needs; and we have assurances from leading experts and labs that we have the capacity to meet this challenge. We must secure mandate and funding to:
- Contain the geographic spread of CWD by enacting and enforcing an immediate ban on the movement of all live cervids, all potentially CWD-infected carcasses, animal parts, products, exposed equipment, trailers, or other sources of infectious materials.
- Mandate and implement for hunters, convenient, cost-free, rapid testing of all animals harvested from CWD-affected areas.
- Ensure that no CWD-infected material reaches the food or feed chains, and that it is instead properly disposed of.
- Establish and fund accountable research and science-based policy to protect public interest (health, wildlife and related industries, agriculture, our economies and communities).
The issues are numerous, serious, and complex, but complacency is not an option. The sooner we act, the greater the prospects to protect our greatest living legacy. Further details, discussion, citations, and scientific references follow.
Potential Risk of Transfer to People There are few considerations which require greater foundational context than questions of zoonotic risk of infectious diseases. Combining public policy and science is very much a matter of addressing uncertain risks that are dynamic, evolving, and with complex, even profound consequences.
The reality is that most (~70%) emerging zoonotic diseases have come from animals.150, 151 Each presented uncertain risks, and in every instance there was a point in history where the animal to human transfer of that particular pathogen had not yet occurred. Such absence of evidence or ‘proof’ can often elicit false inferences that dismiss or underestimate the risk. The UK example of BSE (unexpectedly) transferring to people as vCJD, is but one recent example.152 The impacts were complex, extending far beyond immediate victims, bringing serious and prolonged socioeconomic and health consequences that included suicides tied to the severe economic impacts of BSE on the agricultural economy.153 There are persisting uncertain zoonotic risks related to the BSE that remain to this day. For example, findings in lymphoreticular tissue (archived through appendix samples) indicate that 1 in 2,000 of the UK population are asymptomatic carriers infected with abnormal PrP.154 The long term implications are unknown.
Zoonotic risks are neither static nor merely historic phenomena: “it is estimated that approximately 75 per cent of ‘new’ human pathogens reported in the past 25 years have originated in animals and the risk of zoonoses is predicted to continue to increase.”155 As status quo matters of public policy they require consideration of known and potential consequences. “The Global Burden of Disease Study estimates that, in the year 2000, infectious diseases were responsible for 22% of all deaths and 27% of disability-adjusted life years worldwide.”156
Such risk profiles can only be considered as snapshots in dynamic, evolving landscapes, where observation and evidence of variability—indicating change or evolution—is a vital consideration. This underscores the very essence of the precautionary principle, and nowhere is it more requisite than with respect to infectious pathogens. Inadequate policy or regulatory failures can result in pandemics that kill thousands or even millions of people or other animals, causing enormous damage on economies and ecosystems.
The Precautionary Principle
Where there is a potential for severe or irreversible harm, especially to public wellbeing and interest, an absence of scientific consensus or proof of harm cannot be used to allow or maintain policies or actions underlying the risk. In such cases, the burden to ‘prove safety’ falls on those advocating the potentially harmful policy or action.157
The standard of “severe or irreversible harm” is a very high bar; yet one CWD has long surpassed regarding public wildlife. It is only against that backdrop that the potential transference of CWD to people can be reasonably considered. We must consider risk, consequences, and even worst case scenarios. The fact is that prion diseases are described by physicians and victim’s families as aggressive, horrific, and dreadful.
Faced, in his medical practice, with the reality of human prion and neurodegenerative diseases, a leading scientists like Dr. Neil Cashman, (former) Scientific Director, PrioNet Canada, have long warned that CWD is “an emergency in slow motion.” At the “On The Horizon” PrioNet Research Conference Dr. Cashman summarized the background and urgency as follows:
“CWD is spreading like wildfire. From a few foci in Saskatchewan, it has now come to involve deer and elk in Alberta and Saskatchewan and there are no geographical barriers. It will spread until it infects the entire continent. It also spreads across species. …It can persist in water; it can persist in soil. It’s spreading without check. It’s arguably the most contagious prion disease, and the human health impact is unknown. We just frankly do not know if humans are susceptible to chronic wasting disease. It’s an emergency in slow motion.”158
This combination of growth, spread, changing risk, and extreme consequence explains the near unanimity of caution in available zoonotic analyses: “Although the zoonotic potential of CWD is considered low, identification of multiple CWD strains and the potential for agent evolution upon serial passage hinders a definitive conclusion.”159
Assessing zoonotic risk of new, emerging, and especially fatal diseases, is challenged by the inability to experimentally test susceptibility in people. Indeed, the ethical challenges are formidable enough regarding potential treatments. Yet questions of susceptibility require new approaches combining epidemiological and laboratory analyses (both in vitro and in vivo), as well as considerations of known and probable human exposure. Questions of appropriate policy and regulatory responses must be weighed against all implied consequences (biological, social, and economic), and the entire range of outcomes. This must include potential worst case scenarios even if they are thought extremely unlikely, not just because of evolving risk, but because market, media, and societal responses are often based more on perception than on science or reality.
Experts weigh in
Given their own and the risk analyses of others, leading scientists are expressing concern: “The increasing levels of CWD exposure are highly concerning.” “As a matter of policy, I believe all animals taken from CWD-infected areas should be tested before consumption and people should definitely not be consuming any infected material.”181
Qingzhong Kong, PhD, Case Western Reserve University
“The CWD situation and increasing levels of CWD exposure is a concern for cervid and human public health.” “CWD-testing should be conducted on animals harvested from CWD-infected areas prior to consumption.”182
Candace Mathiason, PhD, Colorado State University
“ … The more opportunity to expose humans to this stuff, the more we’re potentially playing with fire, in terms of these strain adaptations. It wouldn’t take very many cases of human prion disease that were linked back to chronic wasting disease, to where this whole conversation could change, fairly dramatically, and pretty much overnight. So I think while we have the opportunity, to get out in front of this … where we can as best we can, we should probably take advantage of that.”183
Michael Miller, PhD, CO Division of Wildlife
The full spectrum
The scope of human exposure to CWD is broader than is generally appreciated. It includes some direct exposures that have been largely ignored, lessons from history notwithstanding. When early suspicions of BSE being spread through consumption of blood, bone, and nerve tissues were confirmed in 1988,184 it led to bans on feeding meat and bone meal (MBM) supplements.185 Yet the potential risk of CWD in velvet antlers (i.e., blood, bone, and nerve tissue) sold for human consumption continued to be ignored long after both the confirmation of BSE being transferred to people as vCJD,186 and the repeated findings of CWD on game farms.187
A Risk Assessment of TSE products (dated June 2000) undertaken for Health Canada identified “pharmaceutical products containing high risk tissues and elk antler velvet food supplement” as the highest ranking risks.188 Under public pressure the Canadian Food Inspection Agency pledged in October 2000 to destroy velvet antler from CWD-infected animals. However, no recalls nor warnings to potential consumers have ever been issued.189 The difficulty of recalling product widely distributed throughout Asia is accepted; but it also illustrates the challenge and the consequences of failing to detecting potential zoonotic transfer. Furthermore, this passive approach regarding velvet antler continues even after confirmation of PrPd in velvet antler in 2009.190
Why worry?
As evident from challenges in achieving a CWD vaccine for cervids, there is little hope that breakthrough treatments would soon emerge. CWD has been in the shadows; but the toll of other protein misfolding diseases in people (Alzheimer’s, Parkinson’s, Huntington’s, ALS, CreutzfeldtJakob, etc.) affects tens of millions of Americans and cost hundreds of $billions per year. Yet the scale of complexity and level of difficulty is such, that, even after decades of research, there are no cures, and few effective treatments for any of them.191 Moreover, and as with any disease, containing and managing risk of CWD will demand an understanding and acceptance of the relentless capacity of this disease, as it continues to grow, spread, persist, and evolve. “Prions are distinguished from other amyloid diseases both by their infectious character and the observed exponential growth of infectious material.”192
With its growth and spread, human exposure from all sources has been increasing exponentially, and we would do well to consider the implications of both known and unknown factors. For example, prion load has been shown to be relevant, but note the title of McLean and Fryer’s 2011 work “There is No Safe Dose of Prions.” Analysis of 4,338 mice showed “that infection is possible at the very low dose of a 1000-fold dilution of the dose that infects half the challenged animals (ID50).” 193
After pointing out that bank voles (which are circumpolar) are described as the ‘universal acceptor for prions,’ Sigurdson asks if the sequence in the human ?2-?2 loop creates a permissive host PrPC sequence that is converted by prions from other species, despite sequence mismatches.194 With multiple avenues of direct and indirect human exposure, potential bioaccumulation, the potential role of co-factors, stressors, and potentially consequential passage to or through intermediate species, caution remains prudent. Moreover, it’s becoming clear that our understanding will be well served by looking beyond mammals. Quite apart from the work documenting mammalian prions taken up or adhering to plants, Susan Lindquist’s team has recently shown the “first protein from the plant kingdom with bona fide prion attributes.”195
Science, our greatest ally
These analyses outline more than risk: they offer hope. Lindquist has long been at the front of breakthrough prion research with yeast, and has not only documented many collaborative interactions, but key evolutionary and epigenetic analyses to help explain the phenotypic benefits that have conserved prion existence for 800 million years. These and other insights 196 into prion function may well open opportunities to prevent, limit, or potentially even reverse prion disease.197
However hopeful those breakthroughs might be, they are distant, and the levels of human exposure to CWD are already into the UK’s range of 1,000—10,000 BSEinfected carcasses sufficient to result in BSE transferring to a person.198 North American hunter families are consuming some 7,000—15,000 CWD-infected animals per year, and the number is growing exponentially.199 Though deer are much smaller in mass than cattle, this is more than offset by the fact that CWD prions are spread far more broadly than BSE prions in tissues most likely to be consumed.200 Prion load per animal may thus be higher in deer, despite the difference in mass. And while retail markets for beef reach more genetically susceptible consumers, that is less comforting when considering that the entire deer is often consumed by one hunter family.
Overall, the zoonotic risk profile of CWD is complex, uncertain and evolving. Without exception, dozens of experts consulted for this work concur with the current Director, Prion Diseases Program for the Public Health Agency of Canada, Dr. Michael Coulthart, who describes the risk of CWD transferring to people as “far from negligible.”201
Implications are broad, deep, and longterm
What is clear to policy analysts is that even a single transfer of CWD to a person will carry catastrophic implications in reactions of the public, in markets, and in public policy and international trade, regardless of how the disease manifests. And we cannot ignore the reality that CWD is highly contagious in deer.202
It is not inconceivable that a possible transfer to people could result in similar prion shedding in urine, feces, and saliva. Such an occurrence is beyond any known, practical means of containment or treatment, or avenues to curtail the economic fallout. If less dramatic, the risk profile is broad, complex, and with potentially dire outcomes at every turn. As to one minor example: consider the risk of CWD transfer through pet food. That was included in the UK’s updated, March 2016 Qualitative Risk Assessment regarding chronic wasting disease being introduced into Great Britain.203 The assessment asks: What is the risk of CWD being introduced into Great Britain (GB) from North America and causing infection in deer?
The analysis focuses on three routes of potential CWD introduction:
- importation of animal feed
- importation of deer urine lures
- importation of CWD prion on contaminated equipment and clothing/footwear of hunters or other tourists and British servicemen
The assessment cites the European Union Trade Control and Expert System (TRACES), which confirmed that “in November and December 2015, for example, GB imported 13.6112 tonnes of processed cat and dog food (including dog chews) containing products of ungulate origin from Canada and USA.”
The UK Assessment points out that while the U.S. Food and Drug Administration (FDA) recommends that CWD positive deer or elk, or even such considered at risk, may not enter the animal feed system, it is only a recommendation. They therefore conclude that CWD risk material “may constitute a small percentage of the very low tonnage of non-fish origin processed animal proteins imported from the U.S. into GB.” therefore considers that “there is a greater than negligible risk that (nonruminant) animal feed and pet food containing deer and/or elk protein is imported into GB.” (Emphasis in the original.)
As more information becomes known, and major market players get involved, that status quo is unlikely to stay. Pet food regularly includes a variety of rendered animals and animal parts, including road kills. Sept. 15, 2003 the FDA issued guidance that “Material from CWD positive deer and elk may not be used in any animal feed.” That may have seemed a solid precautionary measure, however, Dr. Dave Clausen (from the CWD positive state of Wisconsin) explained that the results soon turned perverse: “Since results of CWD tests would typically take a few days or weeks, renderers in the CWD areas cite this section as the reason to not accept any deer carcasses that have been tested for CWD. Fear was that a positive test would compromise their interest and/or shut down operation. Thus renderers will take untested carcasses just not tested ones.”204
Then, with CWD continuing to extend its range to 24 states and 2 provinces, the FDA recently took further steps, adding a section to cover: “deer and elk considered at high risk for CWD”205 But as the UK Assessment pointed out, this is mere guidance, and does not establish legally enforceable responsibilities.206 Moreover, FDA rules and guidelines for ensuring composition requirements, compliance, monitoring and enforcement are weak, and interstate and international transport of pet foods is widespread and poorly regulated.207
Given their experience with BSE, the UK assessment of risk via pet food is somewhat surprising. Their experience included the world’s first documented instance of interspecies transfer of prion diseases in 1990, when a house cat developed scrapie-like skin irritation so fierce he licked himself bare. Dubbed “Mad Max” by the British press, the cat died from Feline Spongiform Encephalopathy (FSE), a toll eventually reaching 89 domestic cats in UK, one in Northern Ireland, one in Norway, one in Switzerland, and one in Liechtenstein.
Virtually all species of large cats in zoos were similarly infected, including: five cheetahs, three pumas, three ocelots, three tigers, five lions, and one Asian Leopard Cat.208 All were instances of simple oral ingestion of BSEcontaminated feed. The news of transfer across species barriers immediately rocked public confidence and affected markets, which were damaged further with the subsequent admission that people were dying of vCJD from consuming infected beef.209
The UK assessment outlines a similarly “greater than negligible” risk of importation of CWD prion on contaminated equipment and clothing/footwear of hunters, and that “the annual risk of at least one infection of deer in the UK with CWD from deer urine lures imported from the USA is medium.” But whereas official assessments of CWD threats to European wildlife have been measured, largely unseen, and potentially understated, concerns raised by NGOs and the media have been blunt, as in an article in The Times headlined: “Disease from the U.S. could wipe out all the deer in Britain.”210
Any news of international transfer of CWD by any means, to any species whether deer, rodents, pets, or livestock (such as domestic sheep), would almost certainly have severe consequences. The economic implications would be felt most acutely in North American CWD affected areas.
The UK experience with vCJD is instructive, but key differences are noteworthy. Despite recent confirmation of PrPd in saliva of BSE cattle,211 the absence of (efficient) lateral transfer of BSE between living animals limited growth and spread of the disease,212 and it allowed the ruminant feed ban to eventually halt both the epidemic and the subsequent trade embargo. This underscores a contrast of some significance: CWD with its prolific prion shedding in saliva, feces and urine, is a highly contagious, extremely persistent disease, which has established unprecedented reservoirs in public wildlife and the environment. Compared to BSE, CWD offers no apparent ‘off switch.’
Lessons from BSE
From a public policy perspective, the experience with BSE offers vital lessons—from the foundational frame to the conclusions and recommendations by the official inquiry (paraphrased for brevity):
- “At the heart of the BSE story lie questions of how to handle hazard — a known hazard to cattle and an unknown hazard to humans.”
- “BSE developed into an epidemic as a consequence of intensive farming practice(s) … unchallenged over decades, (that) proved a recipe for disaster.”
- “Government was preoccupied with preventing an alarmist over-reaction … (they) believed that the risk was remote. It is now clear that this campaign of reassurance was a mistake.”
- “Public was repeatedly reassured that it was safe to eat beef.” 213
- “Repeated statements that ‘there is no evidence that BSE is transmissible to humans’ does not explain that such evidence would take many years to emerge.”214
- “Even when risk to humans seems remote, all reasonable precautions must be taken.”
- “There should be more checks on possible pathways of transmission, and on occupational risks.”215
- “Where there is uncertainty, government must not shrink from saying “we are not sure.”216
The analyses and recommendations of the UK experience with BSE are founded on failures of governments to uphold public trust and the precautionary principle. The lessons are directly applicable to CWD: Without immediate, science-based intervention by North American governments to contain and limit the spread, growth, evolution, and exposure of CWD, the likelihood of ‘worstcase’ outcomes will continue to increase, and wildlife is in the cross hairs in every scenario.
Monday 15th May 2017
CATTLE IN SPAIN WITH MAD COW DISEASE
On the 28th April 2017 it was confirmed in that cow from Cantabria, Spain born in 2002 (aged 15 years old) was diagnosed with BSE. See report below from the Spanish Government.
Over 50 other animals in the same herd are at risk. The Spanish authorities state that it ‘poses no risk to human health?’ I am afraid that cattle do not develop BSE in isolation, what about the fields these animals have been grazing on? What about the milk and butter that has already gone into the human food chain? Also what about the meat from other animals in the herd which is now in supermarkets and shops?
This diseased cow was 15 years old how long had it been ill?
Human BSE remains a deadly risk for us all and this new case of BSE in Spain, highlights that the disease has not gone away and continues to affect cattle globally and Human BSE continues to kill people.
As the report says below the origins are unknown, so how many other cattle in the area may be suffering from BSE but not showing symptoms when they enter the slaughterhouses?
The report below ends ;THIS EVENT IS RESOLVED’ ??? HOW CAN IT BE RESOLVED BY THE DESTRUCTION OF ONE COW, WHEN 50 PLUS ARE AT RISK AND THE REST OF HERD MAY ALSO BEEN INFECTED.
— SPAIN OIE Bovine Spongiform Encephalopathy atypical L-type Camargo, CANTABRIA
Subject: SPAIN OIE Bovine Spongiform Encephalopathy atypical L-type Camargo, CANTABRIA
| Bovine spongiform encephalopathy , Spain |
Information received on 12/05/2017 from Dr Valentín Almansa, Director General, Sanidad de la Produccion Agraria, Ministerio de Agricultura, Alimentación y Medio Ambiente, Madrid, Spain
| Source of the outbreak(s) or origin of infection |
|
| Epidemiological comments | On April 28th, 2017, the Central Veterinary Laboratory at Algete (National Reference Laboratory for transmissible spongiform encephalopathies accredited under UNE-EN ISO/IEC 17025:2005) received a brainstem sample suspected to be BSE-positive from the regional accredited animal health laboratory of Cantabria (official regional laboratory) after a positive result was obtained through the Bio-Rad TeSeE SAP rapid test. The National Reference Laboratory undertook the confirmatory tests authorized according to Regulation (EU) No. 1148/2014. The selected assays associated were Western blot (Prionics) and ELISA (TeSeE SAP Bio-Rad). Following positive results to both assays, the National Reference Laboratory performed assays to discriminate the BSE strains by immunoblotting with results for atypical BSE type L on May 5th, 2017. The sample was taken within the national TSE surveillance program (sampling of dead or non-slaughtered animals for human consumption over 48 months old). The animal was a crossbred (conjunto mestizo) female born on 25 February 2002. |
Control measures
| Measures applied |
|
| Measures to be applied |
|
Diagnostic test results
| Laboratory name and type | Central Veterinary Laboratory, Algete ( National laboratory ) | ||||||||||||
| Tests and results |
|
Future Reporting
| The event is resolved. No more reports will be submitted. |
WEDNESDAY 19th April 2017
BRAZIL FACES 63 INDICTMENTS FOR YEARS OF UNSAFE TOXIC MEAT FLOODING GLOBAL MARKETS
Huge corruption within Brazils Ministry of Agriculture has meant toxic lethal meat has flooded the global food market for years. Federal Auditors for the Brazilian Government and Ministry of Agriculture at meat processing plants took bribes for years in exchange for false health and safety permits for beef and poultry and domestic animals for human consumption.
63 indictments are being prepared by Brazil’s Federal Police force.
Across Brazil people continue to die of vcjd. These cases of human BSE are all pushed under the carpet by the South American authorities.
Brazil is one of the biggest exporters of meat globally and this corruption means that even more animals w infected with BSE would have also flooded the human food chain for years. JBS the biggest meat packer in the world had one of its staff in Brazil suspended over his involvement with members of the Ministry of Agriculture.
MOY PARK. EUROPES LARGEST POULTRY PROCESSOR WITH 12,000 STAFF ACROSS UK, FRANCE AND NETHERLANDS WAS BOUGHT BY JBS FOR £944 MILLION IN JUNE 2015.
POULTRY GO TO SLAUGHTER BEFORE THEY CAN SHOW SYMPTOMS OF ANY DISEASE INCLUDING THE EQUIVALENT OF BSE.
Mad cow continues to kill people. Food corporations and governments globally profits grow to billions of pounds whilst, thousands of people, young men and women, mums, dads, sisters, grandparents, brothers and children continue to die or suffer the long term lethal effects of the human form of mad cow disease.
Brazil Meat Scandal: 63 Indictments
By Greg Henderson April 17, 2017 | 3:07 pm
Federal Police in Brazil has indicted 63 people for their role in a vast corruption scheme within the Ministry of Agriculture. The charges allege federal auditors at meat processing facilities took bribes for years in exchange for fraudulent sanitary permits.
The probe into Brazil’s meat corruption was launched March 17, 2017, by Brazil’s Federal Police. Brazil, the world’s largest beef and poultry, and the fourth largest exporter of pork, saw its exports drop to near zero within a week of the scandal’s announcement, though most export sales have resumed.
 Andrew just diagnosed with human BSE
Andrew just diagnosed with human BSE
The suspects in the case are charged with falsifying medical records and certificates, tampering with food products, conspiracy and corruption. One employee at a JBS processing plant in Brazil was included in the investigation, allegedly due to his relationship with federal inspectors. The employee was suspended.
Allegations also include selling spoiled meat and injecting water to sell poultry at higher prices. Police also reported that the producers under investigation used ascorbic acid and other chemical ingredients, in quantities far above the legally permitted amount, in order to “disguise the physical aspect or smell of rotten meat.”
No JBS brands or products are associated with product tampering nor has JBS been accused of selling tainted or rotten meat. The majority of this investigation, particularly the food quality issues, focused on the actions of smaller companies in Brazil that supply the domestic market, not JBS.
JBS is the largest meat packer in the world, with subsidiary JBS USA the second largest beef packer in the U.S., with nine beef plants and estimated 2016 sales of $14 billion. JBS USA is not involved in the Brazilian scandal. JBS USA is a “leading processor of beef, pork and lamb in the U.S., a leading processor of beef in Canada and the largest cattle feeder in the world.”
Andrew aged 7 years old at school, happy and healthy
Monday 13th March 2017
A cow born in 2003, over 14 years old has been diagnosed with BSE in Spain March 2017, ( see news links below) this cow produced many calves all of which would have entered either the human food or medicine chain for over a decade.These calves would have been used for milk, butter, meat and in some cases their cells/tissue used for vaccines and blood products. The cow with BSE milk would also have been sold to supermarkets and shops.
There is now a so called ATYPICAL BSE WHICH AUTHORITIES ACROSS THE GLOBE ARE USING TO FUDGE THE TRUE NUMBER OF CATTLE DYING OF MAD COW DISEASE. The authorities falsely reassure the public that ATYPICAL BSE is almost a natural disease in the same way that SPORADIC CJD IS IN HUMANS. Both are falsehoods, dodgy accounting by governments to keep the true numbers of BSE cases in cattle lower and deaths of vcjd the human form of mad cow disease lower in humans.
Before BSE there was no such thing as ATYPICAL BSE IN COWS. This new title for BSE is used to protect the global food and pharmaceutical industries and the farmer in Spain who for over a decade had been selling milk from a cow with BSE, selling the cows offspring for meat and medical use. All of these animal products would have entered the human food and medicine chain.
Its a crude ‘damage limitation’ by the authorities in Spain saying the cow had Atypical BSE. (which means it was an odd case and old before BSE was diagnosed) hoping that the public will believe that ATYPICAL means ‘safe’. Unproven science to falsely reassure the public that beef from this BSE cow from this farm in Spain was and is ‘safe for human consumption’. BSE is lethal to humans and animals, sometimes animals or humans have long incubation periods before they become ill, but they are still toxic to other animals or humans.
This cow which was 14 years old in Spain was found to have BSE and that is a lethal risk to human health. This cow also developed BSE in the same region where a few years ago a mother aged 60 and her son in his 40’s died of vcjd. There have also been other human cases of vcjd in the area of Spain where this cow was recorded as having BSE.
The global cover-up regarding animal BSE and human mad cow disease continues!
ABC NEWS AND OTHER MEDIA REPORTS.
http://www.taylorsvilletimes.com/syndicated_post/spain-reports-case-of-mad-cow-disease/
Cash cows and cover-ups March 2017
Wednesday 1st March 2017
Had two brilliant radio interviews this week, one with presenter Cheryl Fergus-Ferrell at Croydon Radio, London and another with Pippa Jones at TalkRadio Europe which was broadcast across Spain. Both were extended items, talking about my Andrew the campaign and documentary ‘Cash. cows and cover-ups’. See link below to the podcast Croydon Radio.
http://www.croydonradio.com/podcast/show.php?HistoryID=70021a3f-9bf5-ed3e-8ed9-3e03dbb96665
Monday 13th February 2017
We have released a trailer of our shocking new one hour indpendent documentary,
’ Cash, cows and cover-ups’
Please share the link below. I will let you know when the documentary in full is being broadcast. I have worked for over 18 months researching and filming the documentary and have uncovered some shocking new facts and information that the UK government and other establishments wanted to keep secret. Partickular Films are the great production company which has filmed, edited, and directed this great film. It has been produced with passion, professionalism and facts, with many world exclusive revealed. Director Joseph Andrew Mclean, cameramen Martin Heron, Dale McEwan and a great crew in the USA.
We have filmed across the UK and in the USA and the documentary is for release to a national and international audience.
This campaign and film is not just about the unlawful death of my son Andrew and all victims of human BSE but about you and your families. I want to know that the food that children and families in 2017 are eating and the medicines they are ingesting are safe and not a poisoned chalice. Sadly our governments and the global food companies care little for animal or human health with profits the driving force.
If you care about the food you eat, the scientists you put your trust in and the politicians you vote for please watch the trailer and support the documentary when its broadcast.
This concerns everyone, I want to make sure your children are safe, your friends, family and you do not become infected with BSE, do not become disabled or die through human mad cow disease.
‘cash, cows and cover-ups’ and justice4andy campaign is about keeping your family safe too!
The trailer is also on YouTube
https://youtu.be/vRRRC1etgFE
Please circulate
The link is now on Vimeo: https://vimeo.com/203115042
Vimeo: vimeo.com/partickularfilms
Youtube: www.youtube.com/user/PartickularFilms

Monday 6th February 2017
This evening I am appearing on BBC1 ‘INSIDE OUT’ at 7.30pm its a shocking investigation into diseases that can be transmitted from domestic animals to humans. How the UK government in 2017 continue to cut funding regarding testing farm animals for disease and its on-going effect on food safety.
Below is latest research which highlights the on going ticking time-bomb which is human BSE and how millions remain at risk of dying of the human form of mad cow disease.
With this blog is photo of me filming in snowy countryside on a farm. I talk about BSE and my fight to protect the UK and global public from the government/ corporate greed and corruption that unlawfully killed my son Andrew and how BSE will continue to kill people for generations. I also discuss other zoonotic diseases which will flourish all the time government policy condones profit before human health.
Many more people could still die from mad cow disease in the UK

Wednesday 1st February 2017
Roger Hiorns Turner nominated artist has an exhibition of his work at the world famous IKON gallery in Birmingham, UK.
The show is on for 3 months December 2016- March 2017 and includes items from www.justice4andy.com campaign and also Roger’s art expressing the tragedy and corruption surrounding the BSE epidemic and its fatal human consequences. Please go along if you are in the area.
Photo with this blog is of Christine and Roger at his show. My book ‘Who killed my son?’ is also available at the IKONs book store and their catalogue. See link below.
https://ikon-gallery.org/shop/art-books/who-killed-my-son/

Monday January 30th 2017
This footage on Youtube (see below) of a cow staggering and dying of BSE in Belgium , highlights the ticking health-time bomb that is mad cow disease. It has not gone away and is endemic in cattle. With the closing of animal autopsy facilities in England and the UK no longer testing for BSE. How many hundreds of cattle here in the UK and globally are still entering the human food chain that are infected with mad cow disease?
https://www.youtube.com/watch?v=czynqHWkotY
The footage of the cow unable to walk due to deadly mad cow disease and the Belgium officials off-hand response that:
‘Only one cow has BSE’ and that it’s therefore safe and ok for Belgium families and their children to consume bovine material is false. Totally appalling that profit before lives always dominates governments agendas.
BSE in cattle is never isolated to just one case. What about the cows that had already gone to slaughter and not showing symptoms? they would be toxic and infectious too!
How many cows in the Belgium herd were incubating or carrying mad cow disease and entered the human food and medicine chain?
Of course people who consume this toxic material will not show symptoms for many years, by then the farm may well be owned by another farmer and the officials who say eating beef is safe moved on to another post.
All of the cattle in the affected herd should have been immediately destroyed including calves and parents of the cows.
Also all meat and milk that had been sent from the farm should have beentraced and consumers informed.
The culture of global ministerial and official secrecy which killed my son Andrew and hundreds innocent victims, disabled thousands and put millions at risk continues to condone and hide the truth/ facts about BSE and its human on-going deadly consequence vcjd
Photos with this blog of me and my son Andrew aged 24 at Southampton Hospital the day he was diagnosed with human mad cow disease, and 6 months before he died of human BSE. The other photo taken just a short while before of Andrew healthy and well in San Francisco USA.
https://www.youtube.com/watch?v=czynqHWkotY